
Ventolin (GlaxoSmithKline (GSK))
Respiratory & Digestive Treatment
Ventolin (Albuterol) is a fast-acting bronchodilator used as a rescue inhaler to treat and prevent bronchospasm in asthma and COPD.
Table of Contents
Ventolin Product Information
What is Ventolin / Albuterol?
Ventolin, known generically as albuterol in the United States and salbutamol in most of the rest of the world, is a short-acting beta-2 adrenergic receptor agonist (SABA). It is primarily used as a bronchodilator to treat and prevent bronchospasm—the sudden constriction of the muscles in the walls of the bronchioles—in conditions such as asthma and chronic obstructive pulmonary disease (COPD). Administered most commonly via a metered-dose inhaler (MDI), Ventolin provides rapid relief of acute respiratory symptoms, earning it the moniker of a "rescue inhaler."
The active ingredient, albuterol sulfate, works by relaxing the smooth muscles surrounding the airways, allowing them to dilate and facilitating easier airflow into and out of the lungs. Since its introduction to the medical market in the late 1960s, it has become one of the most widely prescribed medications globally, recognized by the World Health Organization (WHO) as an essential medicine due to its critical role in managing acute respiratory distress.
While Ventolin is highly effective for acute symptom relief, it is not a cure for underlying respiratory diseases. It does not address the chronic inflammation that characterizes conditions like asthma. Therefore, it is often prescribed alongside controller medications, such as inhaled corticosteroids, which manage the long-term inflammatory component of the disease.
FDA-Approved Uses and Clinical Indications
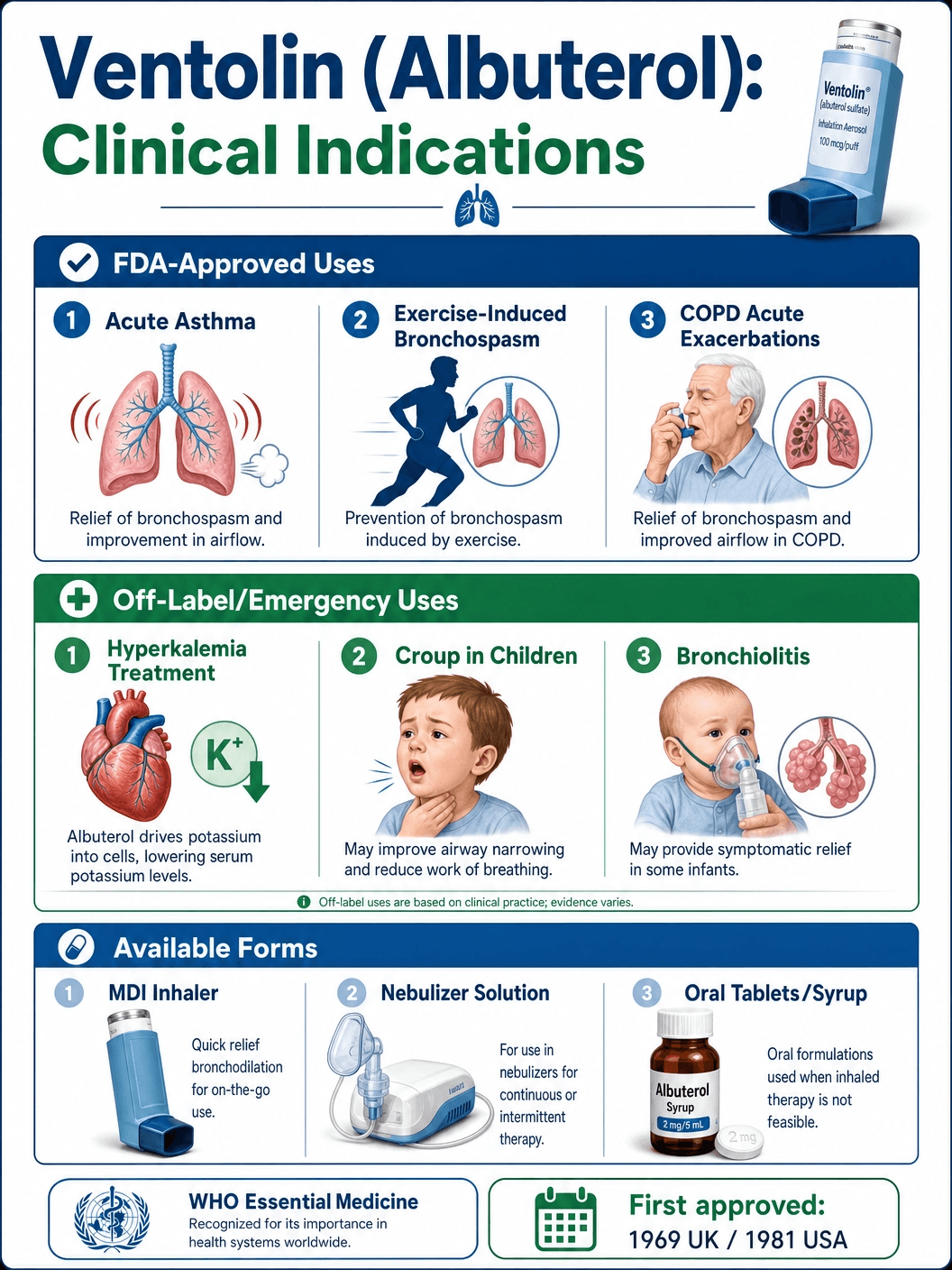
Ventolin is approved by the U.S. Food and Drug Administration (FDA) and other global regulatory bodies for several specific respiratory indications. Its primary use is the treatment or prevention of bronchospasm in patients aged 4 years and older with reversible obstructive airway disease.
Acute Asthma Exacerbations: Ventolin is the first-line treatment for acute asthma attacks. When a patient experiences sudden wheezing, shortness of breath, chest tightness, or coughing, inhaling albuterol provides rapid bronchodilation, usually within minutes. It is the cornerstone of emergency asthma management in both pre-hospital and clinical settings.
Exercise-Induced Bronchospasm (EIB): Many individuals, even those without chronic asthma, experience airway constriction triggered by vigorous physical activity, particularly in cold or dry environments. Ventolin is FDA-approved for the prevention of EIB. When taken 15 to 30 minutes prior to exercise, it effectively blunts the bronchoconstrictive response, allowing patients to participate in physical activities without respiratory distress.
Chronic Obstructive Pulmonary Disease (COPD): While COPD is characterized by largely irreversible airflow limitation, many patients have a reversible component to their airway obstruction. Ventolin is used in COPD management for acute symptom relief, helping to alleviate sudden exacerbations of breathlessness. It is often used in conjunction with long-acting bronchodilators (LABAs or LAMAs) for comprehensive COPD care.
The Mechanism of Action: How Albuterol Opens Airways
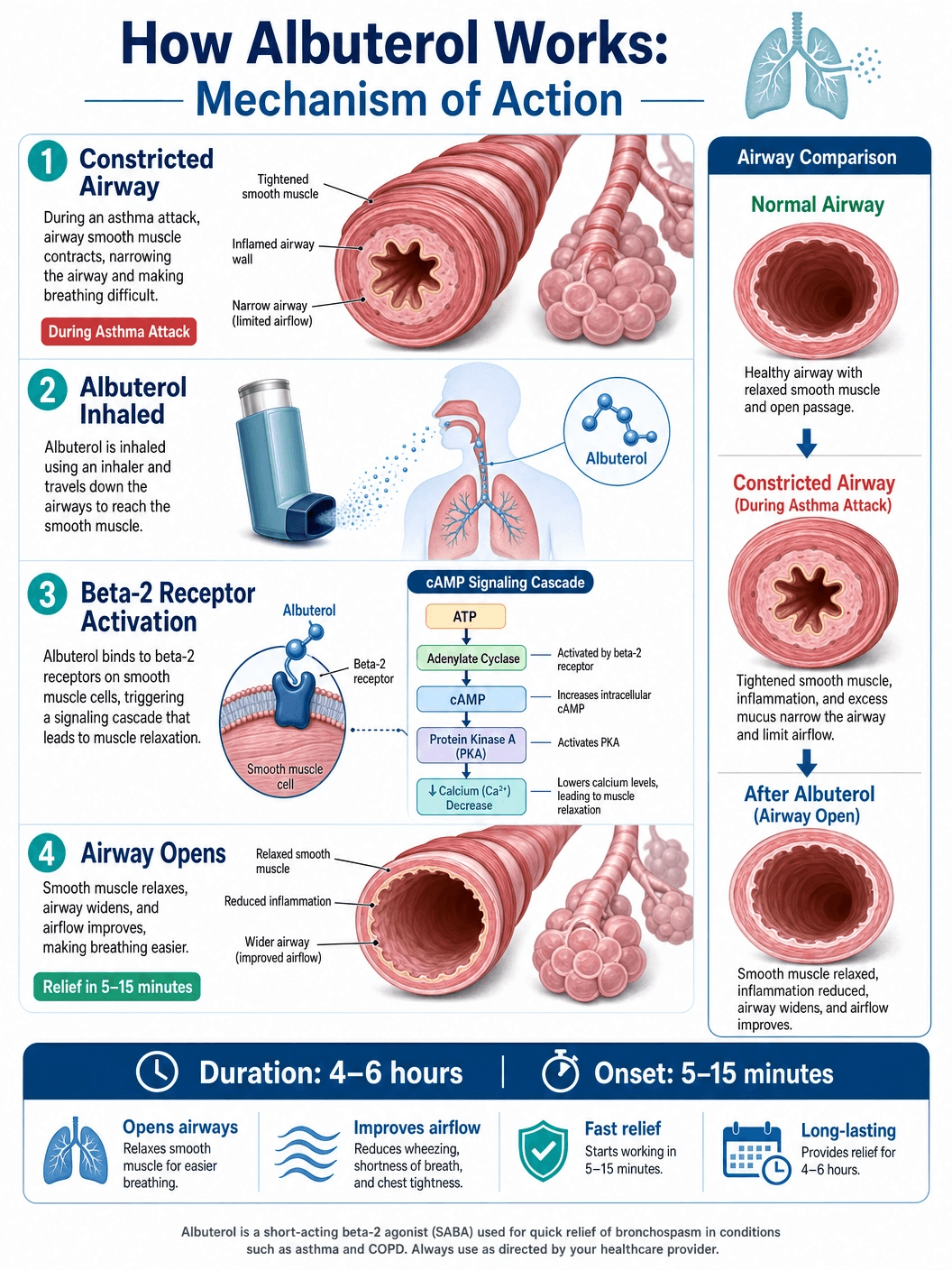
To understand how Ventolin works, one must look at the autonomic nervous system, specifically the sympathetic division, which controls the body's "fight or flight" responses. The smooth muscles lining the bronchioles in the lungs are equipped with beta-2 adrenergic receptors.
When albuterol is inhaled, it travels down the respiratory tract and binds selectively to these beta-2 receptors. This binding activates an intracellular enzyme called adenylate cyclase, which catalyzes the conversion of adenosine triphosphate (ATP) into cyclic adenosine monophosphate (cAMP). An increase in intracellular cAMP levels leads to the activation of protein kinase A, which in turn inhibits the phosphorylation of myosin and lowers intracellular ionic calcium concentrations.
The net result of this biochemical cascade is the relaxation of the bronchial smooth muscle. As the muscles relax, the airways dilate, reducing airway resistance and allowing air to flow more freely. Because albuterol is a "selective" beta-2 agonist, it primarily targets the lungs, with significantly less effect on the beta-1 receptors found in the heart, thereby minimizing (though not entirely eliminating) cardiovascular side effects like tachycardia.
Generic vs. Brand Name Ventolin
The landscape of albuterol inhalers involves both brand-name products and generic equivalents. Ventolin HFA is a specific brand manufactured by GlaxoSmithKline (GSK). However, because the patent for the original albuterol molecule expired decades ago, generic versions are widely available and commonly dispensed.
The HFA Transition: Historically, albuterol inhalers used chlorofluorocarbons (CFCs) as the propellant to deliver the medication into the lungs. Due to environmental concerns regarding ozone depletion, CFC inhalers were phased out globally by 2008. They were replaced by inhalers using hydrofluoroalkane (HFA) propellants. Ventolin HFA was one of the first to make this transition. HFA inhalers deliver the medication with a softer, warmer plume compared to the older CFC inhalers, which sometimes leads patients to mistakenly believe they are not receiving a full dose.
Brand Equivalents: In addition to Ventolin HFA, other brand-name albuterol inhalers include ProAir HFA (Teva) and Proventil HFA (Merck). While the active ingredient (albuterol sulfate) is identical across these brands, the inhaler devices, the specific HFA propellant formulation, and the excipients (inactive ingredients) may vary slightly. Some patients report a preference for the taste or the "feel" of the spray of one brand over another.
Generic Albuterol: Generic albuterol HFA inhalers are therapeutically equivalent to their brand-name counterparts. The FDA requires generics to demonstrate bioequivalence, meaning they deliver the same amount of active drug to the lungs at the same rate. Generics are typically significantly less expensive and are the default choice for most insurance formularies.
Available Dosages and Inhaler Types
Albuterol is available in several formulations, but the metered-dose inhaler (MDI) is the most ubiquitous for outpatient use.
Metered-Dose Inhalers (MDIs)
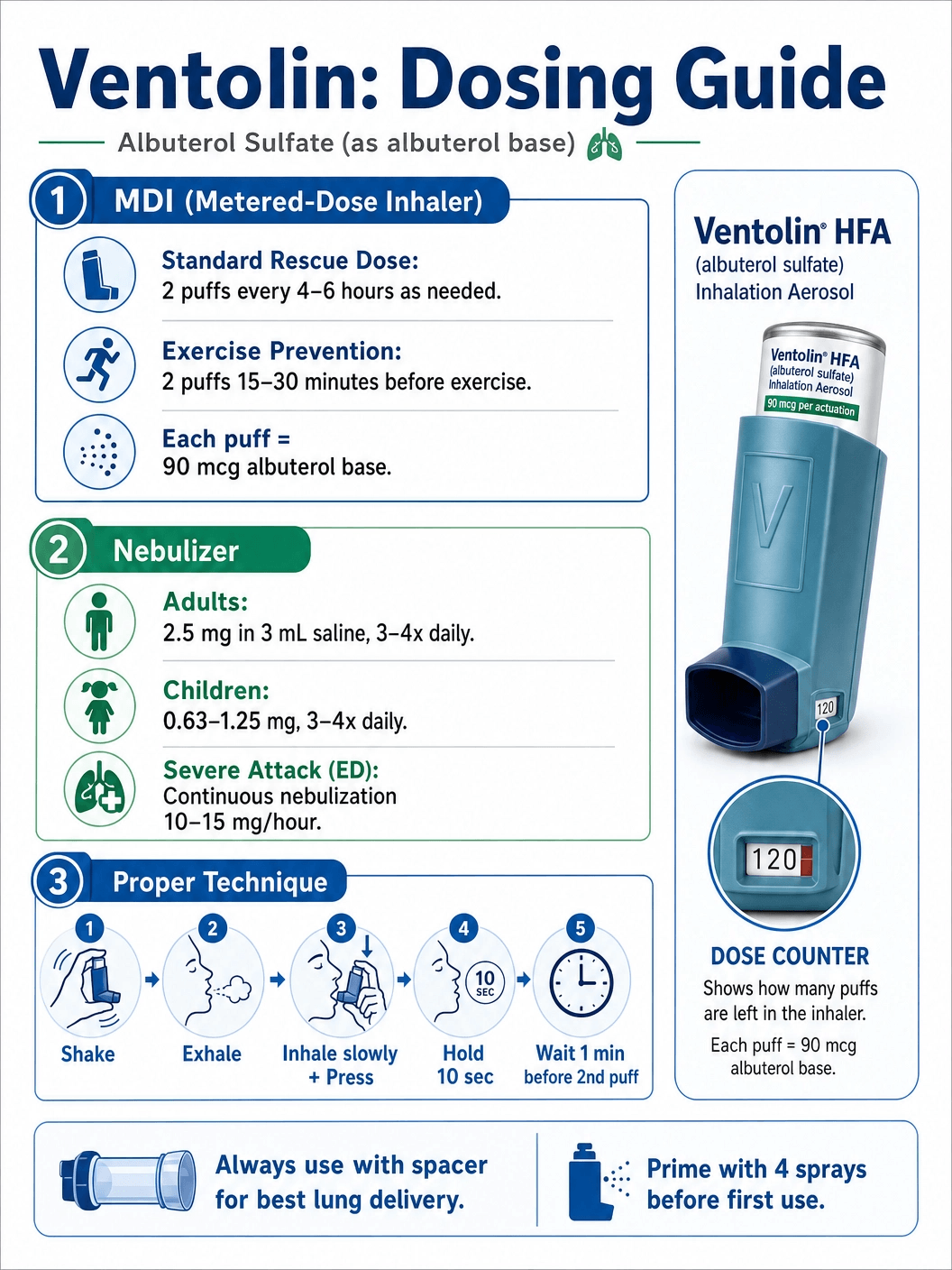
The standard Ventolin HFA inhaler delivers 108 micrograms (mcg) of albuterol sulfate from the mouthpiece per actuation (puff), which is equivalent to 90 mcg of albuterol base. A standard inhaler canister typically contains 200 actuations. The standard adult dose for acute bronchospasm is 2 puffs every 4 to 6 hours as needed. For the prevention of exercise-induced bronchospasm, the dose is 2 puffs taken 15 to 30 minutes before exercise.
Nebulizer Solutions
For patients who cannot effectively use an MDI—such as infants, young children, or patients in severe respiratory distress—albuterol is available as a liquid solution to be used with a nebulizer machine. The nebulizer converts the liquid medication into a fine mist that the patient breathes in through a mask or mouthpiece over 5 to 15 minutes. Standard nebulizer doses for adults are typically 2.5 mg of albuterol administered 3 to 4 times daily as needed.
Oral Formulations
Albuterol is also available in oral forms, including tablets and syrups. However, oral administration is rarely used today because it is less effective than inhaled albuterol and carries a much higher risk of systemic side effects, such as tremors and elevated heart rate. Inhaled albuterol delivers the medication directly to the site of action (the lungs) with minimal systemic absorption.
Proper Inhaler Technique: The Key to Efficacy
The effectiveness of Ventolin is highly dependent on the patient's inhaler technique. Studies consistently show that a significant percentage of patients use their MDIs incorrectly, resulting in the medication depositing in the mouth or throat rather than reaching the lungs.
Standard MDI Technique: The correct steps involve shaking the inhaler well, exhaling completely, placing the mouthpiece between the lips, pressing down on the canister exactly as a slow, deep breath is initiated, and then holding the breath for 10 seconds to allow the medication to settle in the airways.
The Role of Spacers: To overcome coordination difficulties, healthcare providers strongly recommend the use of a valved holding chamber, commonly known as a spacer. A spacer attaches to the inhaler and holds the medication plume in a chamber, allowing the patient to inhale the drug at their own pace. Spacers significantly increase the amount of medication that reaches the lungs and reduce the amount deposited in the mouth, thereby decreasing the risk of side effects like oral thrush (though this is more of a concern with inhaled corticosteroids than with albuterol).
Priming and Cleaning: Ventolin HFA inhalers must be primed before the first use or if they have not been used for more than 14 days. Priming involves spraying 4 test sprays into the air, away from the face, shaking well before each spray. The plastic actuator should also be washed with warm water at least once a week to prevent medication buildup from blocking the spray.
Side Effects and Adverse Reactions
While Ventolin is generally safe and well-tolerated when used as directed, it is a sympathomimetic drug and can cause side effects, particularly if overused.
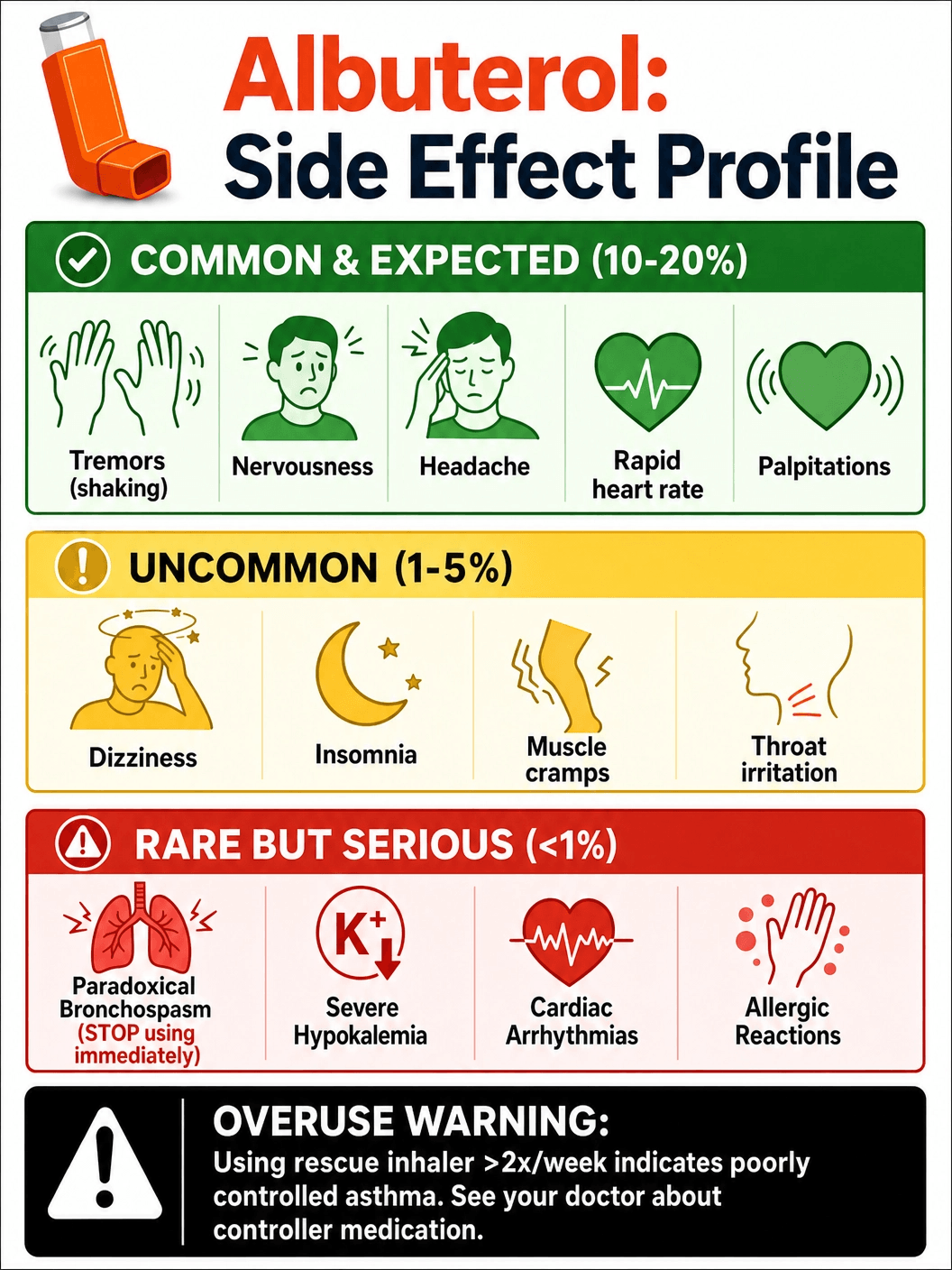
Common Side Effects: The most frequently reported side effects are related to the drug's stimulation of the nervous system. These include fine muscle tremors (especially in the hands), nervousness, jitteriness, and headaches. Some patients may also experience a mild, temporary increase in heart rate (tachycardia) or palpitations. These effects are usually transient and subside as the medication wears off.
Paradoxical Bronchospasm: In rare cases, inhaling albuterol can cause the airways to constrict rather than dilate, a condition known as paradoxical bronchospasm. This is a medical emergency. If a patient experiences sudden worsening of wheezing or shortness of breath immediately after using Ventolin, they should discontinue the inhaler immediately and seek alternative therapy.
Metabolic Effects: High doses of albuterol can cause metabolic changes, most notably hypokalemia (low blood potassium levels). Albuterol drives potassium from the blood into the cells. While usually clinically insignificant at standard doses, it can become problematic in patients taking high doses via nebulizer or those concurrently taking potassium-depleting diuretics. Albuterol can also cause transient increases in blood glucose levels.
The Danger of Over-Reliance: The "Blue Inhaler" Trap
One of the most significant clinical challenges in asthma management is patient over-reliance on SABA inhalers like Ventolin (often recognized by their blue color). Because Ventolin provides rapid, noticeable relief, patients often perceive it as their most important medication.
However, frequent use of Ventolin indicates poorly controlled asthma. If a patient needs to use their rescue inhaler more than twice a week (excluding use for exercise-induced bronchospasm), it is a strong signal that underlying airway inflammation is not being adequately managed. Overuse of SABAs is associated with an increased risk of severe asthma exacerbations, hospitalizations, and even asthma-related mortality.
Current global asthma guidelines, such as those from the Global Initiative for Asthma (GINA), emphasize that SABAs should no longer be used as the sole treatment for asthma. Instead, patients should be prescribed an inhaled corticosteroid (ICS) to address the root cause of the disease—inflammation. The paradigm has shifted toward using a combination ICS-formoterol inhaler as both a daily controller and a rescue medication, reducing the reliance on standalone albuterol inhalers.
Drug Interactions and Precautions
Ventolin can interact with several other medications, requiring careful clinical management.
Beta-Blockers: Beta-adrenergic blocking agents (beta-blockers), commonly used to treat high blood pressure, heart failure, and glaucoma, directly antagonize the effects of albuterol. Non-selective beta-blockers like propranolol can induce severe bronchospasm in asthmatic patients and should generally be avoided. If a beta-blocker is necessary, a cardioselective beta-blocker (e.g., metoprolol) is preferred, though caution is still required.
Diuretics: As mentioned, albuterol can lower blood potassium levels. When used concurrently with non-potassium-sparing diuretics (such as loop diuretics like furosemide or thiazide diuretics), the risk of significant hypokalemia is increased, which can lead to cardiac arrhythmias.
MAOIs and Tricyclic Antidepressants: Ventolin should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors (MAOIs) or tricyclic antidepressants, or within 2 weeks of discontinuation of such agents, because the action of albuterol on the cardiovascular system may be potentiated.
Ventolin in Special Populations
Pediatrics: Ventolin is widely used in pediatric populations for asthma and virus-induced wheezing. For young children, nebulizers or MDIs with a spacer and a well-fitting face mask are essential for effective drug delivery. Parents must be educated on the signs of respiratory distress that warrant emergency medical attention, rather than relying solely on repeated albuterol doses.
Pregnancy and Breastfeeding: Asthma control is crucial during pregnancy, as uncontrolled asthma poses significant risks to the fetus, including hypoxia and low birth weight. Albuterol is generally considered safe for use during pregnancy and is the preferred SABA for pregnant women. It is not known whether albuterol is excreted in human breast milk, but the use of inhaled albuterol is generally considered compatible with breastfeeding due to low systemic absorption.
Geriatrics: Older adults may be more sensitive to the cardiovascular side effects of albuterol, such as tachycardia and tremors. Additionally, elderly patients often have comorbidities like cardiovascular disease or are taking multiple medications (polypharmacy), increasing the risk of drug interactions. Careful monitoring is required.
Purchasing Ventolin: Cost, Insurance, and Legal Acquisition
In the United States and most developed nations, Ventolin and generic albuterol inhalers are prescription-only medications. They cannot be legally purchased over-the-counter (OTC). This regulation ensures that patients with respiratory symptoms are properly evaluated by a healthcare professional to confirm a diagnosis of asthma or COPD and to rule out other serious conditions.
The cost of albuterol inhalers can vary significantly. Brand-name Ventolin HFA can be expensive without insurance coverage. However, generic albuterol HFA is widely available and is typically covered by Medicare, Medicaid, and most private insurance plans, often with a low copayment. Patients without insurance can utilize pharmacy discount cards or manufacturer patient assistance programs to reduce the out-of-pocket cost.
Patients should be wary of online pharmacies offering Ventolin without a prescription. These are often illicit operations selling counterfeit or substandard medications. Counterfeit inhalers may contain incorrect dosages, no active ingredient at all, or harmful propellants, posing a severe risk during an acute asthma attack. Always purchase medications from licensed, reputable pharmacies.
Official Instructions and Guidelines
Patients prescribed Ventolin should adhere strictly to the instructions provided by their healthcare provider and the official prescribing information.
- Do not exceed the recommended dose. If symptoms are not relieved by the prescribed dose, or if they worsen rapidly, seek immediate emergency medical care.
- Keep track of usage. Many modern inhalers, including Ventolin HFA, feature a built-in dose counter. Patients should monitor this counter and request a refill when the numbers turn red (usually at 20 doses remaining) to ensure they are never without rescue medication.
- Store properly. The inhaler should be stored at room temperature, away from extreme heat or cold. The canister is pressurized and can burst if exposed to high temperatures (e.g., left in a hot car). Do not puncture or incinerate the canister.
- Maintain an Asthma Action Plan. Every patient with asthma should have a written Asthma Action Plan developed with their doctor. This plan details when to use Ventolin, when to increase controller medications, and when to seek emergency help based on symptoms or peak flow meter readings.
Government and Regulatory Resources
For the most accurate, up-to-date, and comprehensive information regarding Ventolin (albuterol), patients and healthcare professionals should consult official government and medical organization resources:
- U.S. Food and Drug Administration (FDA): The FDA provides access to the official, approved prescribing information (drug label) for Ventolin HFA, detailing all clinical pharmacology, contraindications, and clinical trial data.
- National Institutes of Health (NIH) / MedlinePlus: MedlinePlus offers patient-friendly, easy-to-understand information on albuterol oral inhalation, including how to use the inhaler properly and what side effects to watch for.
- Global Initiative for Asthma (GINA): GINA publishes globally recognized, evidence-based strategy documents for asthma management and prevention, outlining the appropriate role of SABAs like albuterol in modern asthma care.
- Centers for Disease Control and Prevention (CDC): The CDC provides extensive public health information on asthma prevalence, triggers, and management strategies.
The Evolution of Albuterol: From Discovery to Modern Use
The story of albuterol is a fascinating chapter in the history of pharmacology, representing a significant leap forward in the treatment of respiratory diseases. Before the 1960s, the primary bronchodilators available were non-selective beta-agonists like isoprenaline (isoproterenol). While effective at opening airways, isoprenaline stimulated both beta-1 receptors (found primarily in the heart) and beta-2 receptors (found in the lungs). This lack of selectivity meant that patients often experienced severe cardiovascular side effects, including dangerous spikes in heart rate and arrhythmias, alongside their respiratory relief.
In the late 1960s, a team of researchers at Allen & Hanburys (which later became part of GlaxoSmithKline) in the United Kingdom, led by Sir David Jack, set out to find a safer alternative. Their goal was to synthesize a molecule that would selectively target the beta-2 receptors in the lungs while sparing the beta-1 receptors in the heart. Through meticulous chemical modification of the isoprenaline molecule, they discovered salbutamol (albuterol). This new compound demonstrated a high degree of beta-2 selectivity, providing potent bronchodilation with a vastly improved cardiovascular safety profile.
Salbutamol was first launched in the UK in 1969 under the brand name Ventolin. It quickly revolutionized asthma care, replacing older, more dangerous medications. It was approved by the FDA for use in the United States in 1981 under the generic name albuterol. Today, over fifty years after its discovery, it remains the most widely prescribed bronchodilator in the world, a testament to the enduring impact of this pharmacological breakthrough.
Albuterol in the Emergency Department
When a patient arrives at the emergency department (ED) in the throes of a severe asthma exacerbation or a COPD flare-up, albuterol is almost always the first medication administered. The clinical presentation of such an emergency is dramatic: the patient is often gasping for air, unable to speak in full sentences, visibly using accessory muscles in their neck and chest to breathe, and producing a high-pitched wheezing sound.
In this critical setting, albuterol is typically delivered via a continuous or frequent intermittent nebulizer treatment rather than a standard MDI. The nebulizer allows for a higher, sustained dose of the medication to be delivered directly into the lungs over a period of time. The rapid onset of action—often within 5 to 15 minutes—can be life-saving, reversing the severe bronchospasm and preventing respiratory failure.
However, emergency physicians know that albuterol alone is not enough for a severe attack. While it opens the airways, it does nothing to stop the massive inflammatory cascade that triggered the attack in the first place. Therefore, ED protocols dictate that systemic corticosteroids (such as oral prednisone or intravenous methylprednisolone) be administered concurrently with albuterol. The albuterol provides immediate rescue, while the steroids take several hours to begin reducing the underlying inflammation, preventing a relapse once the albuterol wears off.
The Environmental Impact of Inhalers
The transition from CFC to HFA propellants in the early 2000s was a major environmental victory, significantly reducing the ozone-depleting potential of medical inhalers. However, the environmental story of inhalers does not end there. While HFAs do not destroy the ozone layer, they are potent greenhouse gases with a high global warming potential (GWP). The HFA propellants used in MDIs like Ventolin contribute to climate change, albeit on a much smaller scale than industrial emissions.
This realization has sparked a new wave of innovation and environmental consciousness within the pharmaceutical industry and the medical community. There is a growing push to transition patients, when clinically appropriate, from pressurized MDIs to dry powder inhalers (DPIs) or soft mist inhalers (SMIs). DPIs and SMIs do not use chemical propellants; instead, they rely on the patient's own inhalation effort or a mechanical spring to deliver the medication. These devices have a near-zero carbon footprint compared to MDIs.
However, this transition is not simple. MDIs remain the most cost-effective option in many regions, and they are essential for patients who cannot generate the strong, deep breath required to use a DPI effectively, such as young children, the elderly, or those in the midst of a severe asthma attack. The medical community is currently balancing the need for effective, accessible respiratory care with the imperative to reduce the carbon footprint of healthcare.
Albuterol and Sports: The Anti-Doping Perspective
The use of albuterol by competitive athletes is a subject of strict regulation by anti-doping agencies, including the World Anti-Doping Agency (WADA). Because albuterol is a beta-2 agonist, it has the potential to act as a performance-enhancing drug. In high, systemic doses (such as those achieved through oral tablets or injections), beta-2 agonists can have an anabolic effect, increasing muscle mass and decreasing body fat, similar to the effects of clenbuterol.
However, inhaled albuterol, when used at therapeutic doses for the treatment of asthma or exercise-induced bronchospasm, does not provide these anabolic benefits. WADA recognizes that many elite athletes suffer from asthma—in fact, the prevalence of asthma is often higher among endurance athletes than in the general population due to the chronic stress placed on their airways.
Therefore, WADA permits the use of inhaled albuterol, but with strict limitations. Athletes are allowed to inhale a maximum of 1600 micrograms over 24 hours, in divided doses not to exceed 800 micrograms over 12 hours starting from any dose. If an athlete's urine sample shows a concentration of albuterol exceeding 1000 nanograms per milliliter, it is presumed not to be the result of therapeutic inhaled use and is considered an Adverse Analytical Finding (a positive doping test), unless the athlete can prove through a controlled pharmacokinetic study that the abnormal result was the consequence of the use of a therapeutic dose of inhaled albuterol.
Understanding the "SMART" Therapy Paradigm Shift
For decades, the standard approach to mild asthma was to prescribe an albuterol inhaler to be used "as needed" for symptom relief. However, this approach has been fundamentally challenged by recent massive clinical trials and subsequent changes to global guidelines.
The problem with the "albuterol-only" approach is that it treats the symptom (bronchospasm) while ignoring the disease (airway inflammation). Patients using only albuterol remain at risk for severe, life-threatening exacerbations. To address this, the Global Initiative for Asthma (GINA) introduced a paradigm shift known as SMART (Single Maintenance and Reliever Therapy).
In the SMART approach, patients do not use a standalone albuterol inhaler. Instead, they use a single inhaler containing a combination of an inhaled corticosteroid (ICS) and a fast-acting, long-lasting beta-agonist (formoterol). They use this single inhaler both for daily maintenance (to control inflammation) and for rescue relief when symptoms occur. When they take a puff for rescue, they get immediate bronchodilation from the formoterol, but crucially, they also get an extra dose of the anti-inflammatory steroid right when the airways are starting to flare up.
This strategy has been shown to significantly reduce the risk of severe asthma attacks compared to using albuterol alone. While Ventolin remains a critical medication for emergency situations and for patients whose asthma is well-controlled on other regimens, the era of prescribing albuterol as the sole therapy for asthma has officially ended in modern clinical practice.
Albuterol Toxicity and Overdose Management
While albuterol is generally safe when used at therapeutic doses, accidental or intentional overdose can lead to significant toxicity. Because albuterol is a sympathomimetic amine, an overdose essentially throws the body's "fight or flight" system into overdrive. The clinical presentation of albuterol toxicity is an exaggeration of its known side effects, but at a much more dangerous level.
Clinical Presentation: A patient presenting with albuterol toxicity will typically exhibit profound tachycardia (a resting heart rate often exceeding 140 beats per minute), severe tremors, agitation, and diaphoresis (excessive sweating). They may complain of chest pain or palpitations. In severe cases, the cardiovascular stimulation can lead to arrhythmias, hypertension followed by hypotension, and even cardiac arrest.
Metabolic Derangements: The most critical metabolic consequence of albuterol overdose is severe hypokalemia. The massive stimulation of beta-2 receptors drives potassium from the extracellular fluid into the intracellular space. This rapid drop in blood potassium levels further increases the risk of fatal cardiac arrhythmias. Additionally, the overdose can cause lactic acidosis and hyperglycemia.
Management: There is no specific antidote for albuterol. Treatment is primarily supportive and symptomatic. In the emergency department, the patient will be placed on continuous cardiac monitoring. Intravenous fluids are administered, and potassium levels are closely monitored and aggressively replaced via IV if hypokalemia is severe. In cases of life-threatening tachycardia or arrhythmias, a cardioselective beta-blocker (like metoprolol or esmolol) may be administered cautiously to counteract the beta-adrenergic stimulation, though this carries the risk of inducing severe bronchospasm, especially in asthmatic patients.
The Role of Albuterol in Hyperkalemia Treatment
Interestingly, the very mechanism that causes a dangerous side effect in overdose—the shifting of potassium into cells—is utilized therapeutically in a completely different medical emergency: hyperkalemia (dangerously high blood potassium levels). Hyperkalemia is a life-threatening condition most commonly seen in patients with severe kidney disease, and it can cause sudden cardiac death.
When a patient presents with severe hyperkalemia, emergency physicians use a multi-pronged approach to lower the potassium levels quickly. One of the standard treatments is the administration of high-dose nebulized albuterol (typically 10 to 20 mg, which is 4 to 8 times the standard asthma dose). The massive dose of albuterol rapidly stimulates the Na+/K+-ATPase pump on cell membranes, forcing potassium out of the blood and into the cells, temporarily lowering the serum potassium concentration and protecting the heart.
It is important to note that albuterol does not remove potassium from the body; it merely hides it inside the cells. Therefore, it is used as a temporary stabilizing measure alongside other treatments (like insulin and glucose, or dialysis) that actually eliminate the excess potassium from the body.
Albuterol in Veterinary Medicine
The pharmacological principles of albuterol apply not only to humans but also to many animal species, making it a valuable tool in veterinary medicine. Just as in humans, animals can suffer from reactive airway diseases that cause bronchospasm and respiratory distress.
Feline Asthma: Cats are particularly prone to a condition known as feline asthma, which presents very similarly to human asthma, with coughing, wheezing, and acute respiratory distress. Veterinarians frequently prescribe albuterol for cats experiencing an acute asthma attack. Because cats cannot use a standard inhaler, the medication is delivered using a specialized feline aerosol chamber (such as the AeroKat) that attaches to the MDI and fits over the cat's nose and mouth.
Equine Recurrent Airway Obstruction (RAO): Horses can suffer from a condition formerly known as "heaves," now termed Equine Asthma or RAO. This is an allergic respiratory disease triggered by environmental dust and molds found in hay and stables. Albuterol, often administered via a specialized equine inhaler mask, is used to provide rapid relief of bronchospasm in horses experiencing an acute flare-up, allowing them to breathe easier while environmental management and corticosteroids address the underlying inflammation.
Canine Bronchitis: While true asthma is rare in dogs, they can suffer from chronic bronchitis or allergic airway disease. Albuterol may be used as a bronchodilator in these cases, though its use is less common than in cats or horses. Veterinarians must carefully monitor animals receiving albuterol for signs of toxicity, which mirror human symptoms: extreme restlessness, elevated heart rate, and tremors.
The Pharmacokinetics of Albuterol: Absorption, Distribution, and Elimination
Understanding how the body processes albuterol is crucial for optimizing its therapeutic use and minimizing side effects. The pharmacokinetics of albuterol vary significantly depending on the route of administration.
Inhalation vs. Oral Administration: When albuterol is inhaled via an MDI, only about 10% to 20% of the dose actually reaches the lower airways. The remaining 80% to 90% is deposited in the oropharynx (mouth and throat) and is subsequently swallowed. The portion that reaches the lungs acts locally on the beta-2 receptors, providing rapid bronchodilation within 5 to 15 minutes. This local action is why inhaled albuterol is so effective with relatively low systemic side effects.
The swallowed portion of the inhaled dose, along with any orally administered albuterol (tablets or syrup), is absorbed from the gastrointestinal tract. However, it undergoes significant "first-pass metabolism" in the liver. The liver rapidly converts a large portion of the albuterol into an inactive sulfate conjugate before it ever reaches the systemic circulation. This is why oral doses of albuterol must be much higher than inhaled doses to achieve the same effect, and why oral administration is associated with a much higher incidence of systemic side effects like tremors and tachycardia.
Distribution and Half-Life: Once in the systemic circulation, albuterol does not bind strongly to plasma proteins (only about 10%). It is widely distributed throughout the body, crossing the blood-brain barrier and the placenta. The elimination half-life of albuterol—the time it takes for the concentration of the drug in the blood to decrease by half—is approximately 3.8 to 6 hours. This relatively short half-life explains why the therapeutic effects of a standard Ventolin dose wear off after 4 to 6 hours, necessitating repeated dosing during an acute exacerbation.
Excretion: Albuterol and its inactive metabolites are excreted primarily by the kidneys in the urine. Approximately 72% of an inhaled dose is excreted in the urine within 24 hours, with about 30% as unchanged active drug and the rest as the inactive sulfate conjugate. A small amount (less than 10%) is excreted in the feces. Because it is cleared by the kidneys, patients with severe renal impairment may experience a prolonged half-life and an increased risk of toxicity, though this is rarely a clinical issue with standard inhaled doses.
Navigating the Transition: CFC to HFA and Beyond
The transition from chlorofluorocarbon (CFC) propellants to hydrofluoroalkane (HFA) propellants in the early 2000s was a monumental shift in respiratory medicine, driven entirely by environmental mandates rather than clinical necessity. The Montreal Protocol, an international treaty designed to protect the ozone layer, mandated the phase-out of CFCs, forcing the pharmaceutical industry to reformulate every MDI on the market.
This transition was not without its challenges. The new HFA propellants had different physical properties than CFCs. They required new canister designs, new metering valves, and new excipients (such as ethanol or oleic acid) to keep the albuterol in suspension or solution. When Ventolin HFA and other HFA inhalers were first introduced, many patients complained that the new inhalers "didn't work."
The primary reason for this perception was the difference in the spray plume. CFC inhalers delivered a forceful, cold blast of medication that patients could clearly feel hitting the back of their throats. HFA inhalers, in contrast, deliver a softer, warmer, and slower-moving plume. Because patients couldn't feel the forceful impact, they assumed they weren't getting the medicine. Extensive patient education was required to reassure them that the softer HFA plume was actually more effective at reaching the small airways of the lungs, rather than just coating the back of the throat.
Furthermore, HFA inhalers are more prone to clogging than the old CFC inhalers. The medication can build up around the tiny opening in the plastic actuator. This necessitated new instructions for patients to wash the plastic actuator with warm water at least once a week—a step that was rarely necessary with CFC inhalers. Today, the HFA transition is complete, but the industry is already looking ahead to the next generation of propellants with even lower global warming potential, ensuring that the evolution of the rescue inhaler continues.
Ventolin Quick View
| Manufacturer | GlaxoSmithKline (GSK) |
|---|---|
| Type | Short-Acting Beta-2 Agonist (SABA) |
| Prescription | Required |
| Pregnancy Category | Category C |
| Alcohol Interaction | No direct interaction, but alcohol can trigger asthma symptoms in some individuals. |
Ventolin Side Effects
Common Side Effects
- Tremors (especially in the hands)
- Nervousness or jitteriness
- Headache
- Rapid heart rate (tachycardia)
- Palpitations
Uncommon Side Effects
- Dizziness
- Insomnia
- Muscle cramps
- Dry mouth or throat irritation
Rare Side Effects
- Paradoxical bronchospasm (sudden worsening of breathing)
- Severe hypokalemia (low potassium)
- Cardiac arrhythmias
- Allergic reactions (rash, hives, swelling)
Important Warning: WARNING: Frequent use of Ventolin (more than twice a week for symptom relief) indicates poorly controlled asthma. Do not rely solely on a rescue inhaler. Consult your doctor about adding an inhaled corticosteroid controller medication.
More Information About Ventolin
Storage
Store at room temperature with the mouthpiece down. Keep away from extreme heat or open flame, as the pressurized canister may burst.
Contraindications
Drug Interactions
Ventolin FAQs
Written and Reviewed by Our Qualified Team

Find out more about our medical content authors and how we ensure the accuracy of our content.
Content last updated: 20 May 2024
Ventolin Reviews
Based on 0 reviews
Leave a Review
How Does It Work?
Research
Read our comprehensive review to understand the medication
Consult Your Doctor
Discuss the medication with your healthcare provider
Get Your Prescription
Obtain a valid prescription from your doctor