
Prednisolone (Orapred, Pediapred, Millipred)
General Health Treatment
The definitive medical guide to Prednisolone: clinical applications, the critical difference from prednisone, safety protocols, tapering guidelines, and comprehensive patient education.
Table of Contents
Prednisolone Product Information
What is Prednisolone?
Prednisolone is a highly potent, synthetic glucocorticoid (a type of corticosteroid) that is widely used in human and veterinary medicine for its profound anti-inflammatory and immunosuppressive properties. It is a derivative of cortisol, the natural stress hormone produced by the adrenal glands, but it has been chemically modified to be significantly more powerful and to have a longer duration of action.
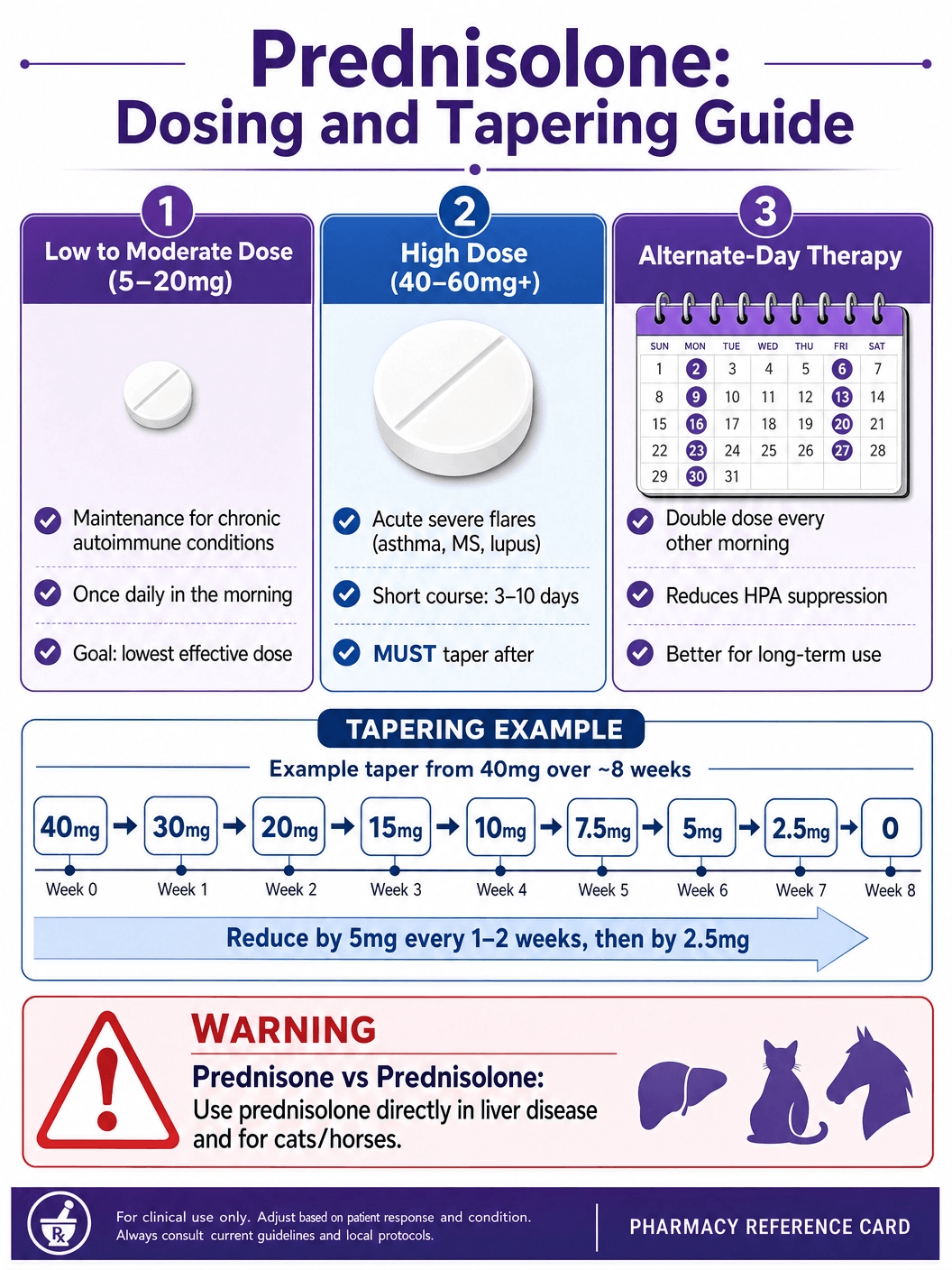
It is crucial to understand the relationship between prednisolone and its closely related counterpart, prednisone. Prednisone is a "prodrug," meaning it is biologically inactive when swallowed. Once it reaches the liver, an enzyme called 11-beta-hydroxysteroid dehydrogenase converts it into prednisolone, which is the active form that actually exerts the therapeutic effects in the body. Therefore, taking prednisolone directly bypasses the need for hepatic conversion. This makes prednisolone the preferred choice for patients with severe liver disease (who may not be able to efficiently convert prednisone) and for veterinary use in cats and horses, which lack the necessary enzymes to process prednisone effectively.
Mechanism of Action: How Prednisolone Works
Prednisolone works at the cellular and genetic levels to suppress inflammation and modulate the immune system. Its mechanism of action is complex and multifaceted, affecting almost every organ system in the body.
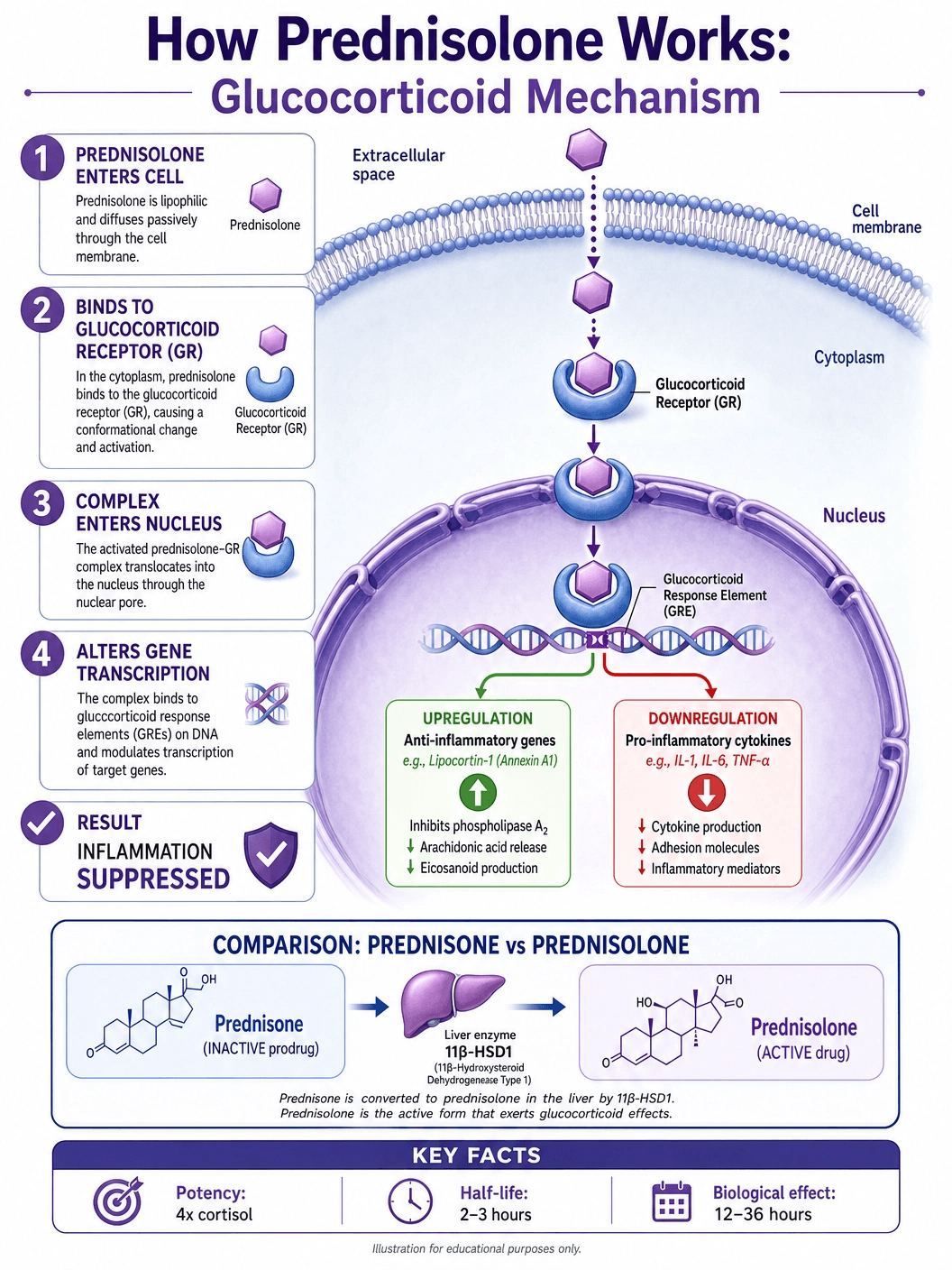
Cellular Entry and Receptor Binding: Because it is a steroid hormone, prednisolone is highly lipophilic (fat-soluble). This allows it to easily pass through the cell membrane of almost any cell in the body. Once inside the cytoplasm, it binds to specific glucocorticoid receptors (GRs). This binding causes the receptor to change its shape and shed protective proteins, activating the receptor-steroid complex.
Gene Transcription (Genomic Effects): The activated complex then moves into the cell's nucleus, where it binds directly to specific sequences of DNA known as glucocorticoid response elements (GREs). This interaction alters the transcription of hundreds of genes. Prednisolone upregulates (increases the production of) anti-inflammatory proteins, such as lipocortin-1, which inhibits the production of inflammatory mediators like prostaglandins and leukotrienes. Simultaneously, it downregulates (decreases the production of) pro-inflammatory cytokines, such as interleukin-1 (IL-1), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-alpha).
Non-Genomic Effects: In addition to altering gene expression (which takes hours to days to take full effect), prednisolone also exerts rapid, non-genomic effects. It can quickly alter the function of cell membranes and ion channels, leading to an immediate reduction in capillary permeability. This rapid action is what stops the leakage of fluid into tissues, quickly reducing swelling and edema in acute inflammatory crises.
FDA-Approved Uses and Clinical Indications
Prednisolone is approved for the treatment of a vast array of conditions characterized by excessive inflammation or an overactive immune system. It is rarely a cure; rather, it is used to control symptoms and prevent tissue damage while the underlying disease is addressed or goes into remission.
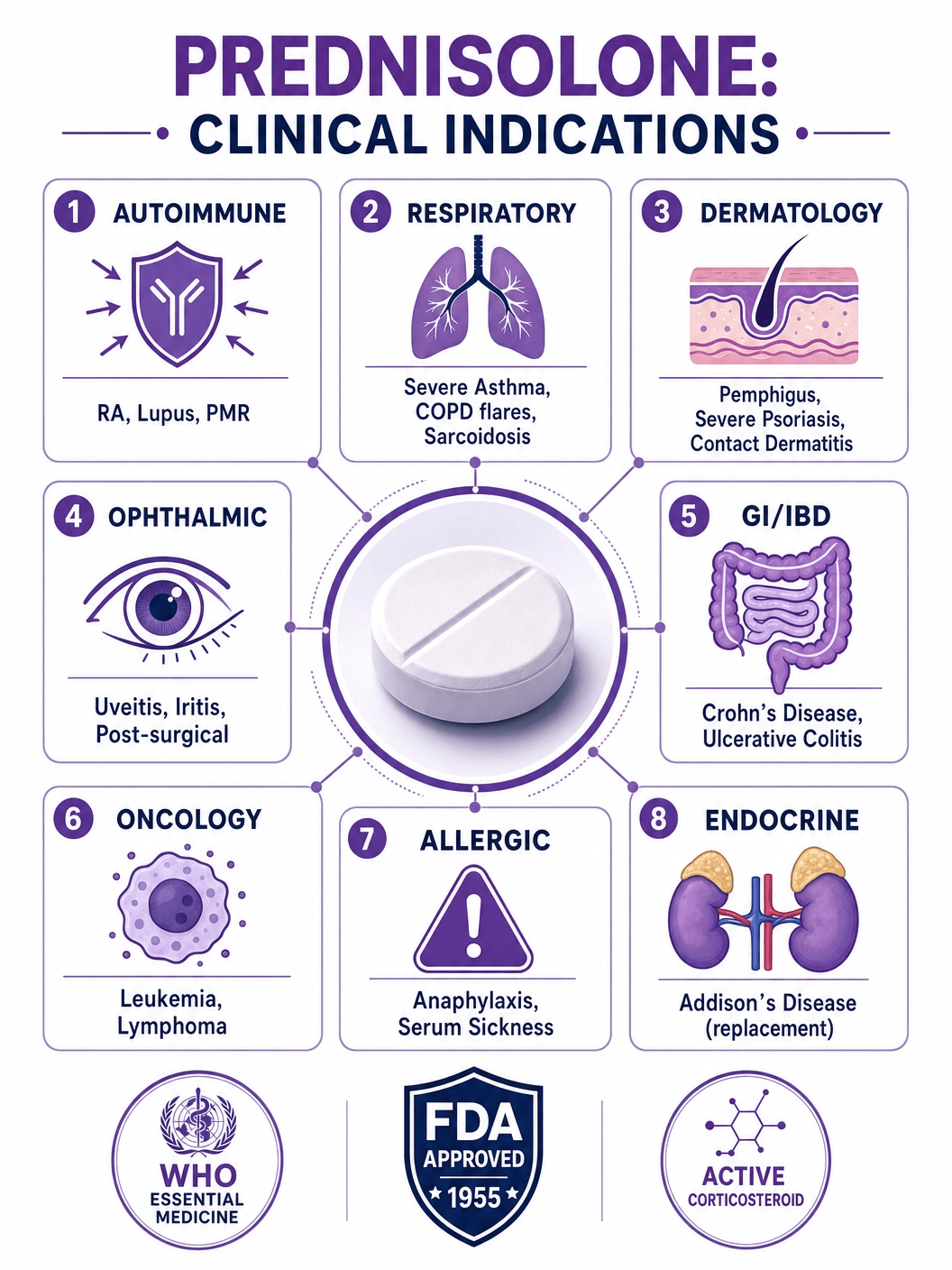
Endocrine Disorders: It is used as replacement therapy in patients with primary or secondary adrenocortical insufficiency (Addison's disease), where the body cannot produce enough of its own cortisol.
Rheumatic and Autoimmune Diseases: Prednisolone is a cornerstone in the management of acute exacerbations of rheumatoid arthritis, systemic lupus erythematosus (SLE), ankylosing spondylitis, and polymyalgia rheumatica. It rapidly reduces joint swelling, pain, and stiffness.
Respiratory Conditions: It is critical in treating severe asthma exacerbations, chronic obstructive pulmonary disease (COPD) flare-ups, and symptomatic sarcoidosis. By reducing airway inflammation, it quickly restores breathing capacity.
Dermatological Diseases: Severe, acute skin conditions such as pemphigus, severe psoriasis, Stevens-Johnson syndrome, and severe contact dermatitis (like extreme poison ivy reactions) are often treated with systemic prednisolone to halt the inflammatory cascade.
Allergic States: It is used for severe or incapacitating allergic conditions that do not respond to conventional treatments, including serum sickness, severe seasonal allergies, and drug hypersensitivity reactions.
Ophthalmic Diseases: Severe acute and chronic allergic and inflammatory processes involving the eye, such as uveitis, iritis, optic neuritis, and allergic conjunctivitis, are frequently treated with prednisolone (often in the form of eye drops, but systemically for severe cases).
Gastrointestinal Diseases: It is used to induce remission in inflammatory bowel diseases (IBD), specifically Crohn's disease and ulcerative colitis, during acute flare-ups.
Neoplastic Diseases: Prednisolone is an integral part of chemotherapy regimens for certain cancers, particularly leukemias and lymphomas (such as acute lymphocytic leukemia and Hodgkin's lymphoma), due to its ability to induce apoptosis (programmed cell death) in lymphoid cells.
Prednisolone vs. Prednisone: The Hepatic Connection
The distinction between prednisolone and prednisone is one of the most frequently misunderstood aspects of corticosteroid therapy. While they are often used interchangeably in clinical practice for healthy adults, the difference is pharmacologically significant.
The Prodrug Concept: As mentioned, prednisone is a prodrug. It has no intrinsic biological activity. To become active, it must pass through the liver, where the enzyme 11-beta-hydroxysteroid dehydrogenase type 1 (11β-HSD1) reduces the ketone group at the C11 position to a hydroxyl group, converting it into prednisolone.
When Prednisolone is Mandatory: In a healthy individual, this conversion happens rapidly and efficiently, making the two drugs essentially equivalent in terms of dosing and effect. However, in patients with severe hepatic impairment (such as cirrhosis or severe hepatitis), the liver's ability to perform this conversion is compromised. If such a patient is given prednisone, they may not achieve therapeutic blood levels of the active drug. Therefore, patients with significant liver disease must be prescribed prednisolone directly to ensure they receive the intended anti-inflammatory effect.
Understanding the Side Effect Profile
The side effects of prednisolone are directly related to the dose and the duration of therapy. Short courses (less than two weeks) are generally well-tolerated, but long-term use carries significant risks that require careful medical management.
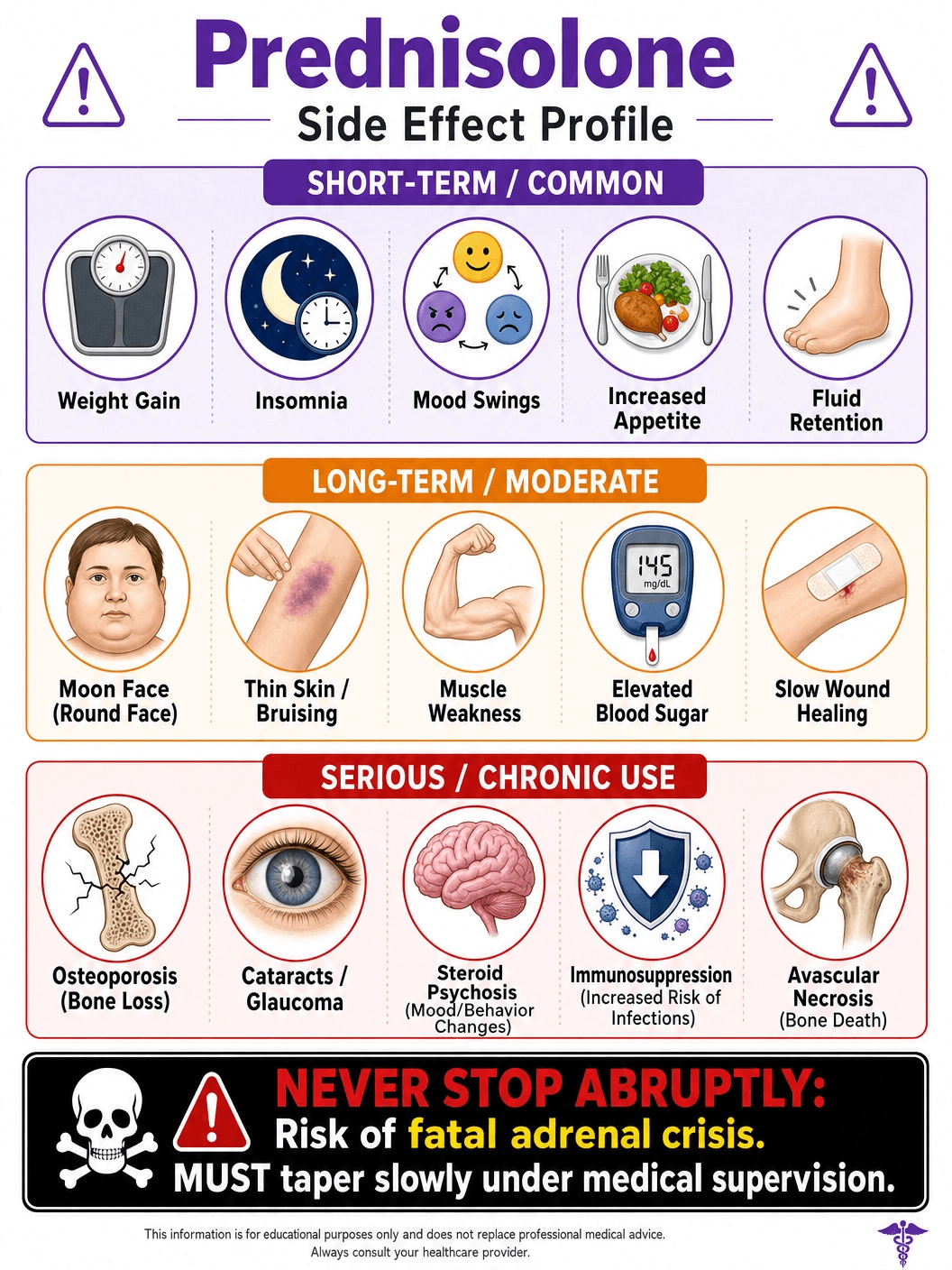
Short-Term Side Effects: Even with brief courses, patients frequently experience increased appetite, weight gain, fluid retention (leading to swelling in the face and ankles), insomnia, and mood changes (ranging from mild euphoria to severe anxiety or irritability). It can also cause a temporary spike in blood sugar levels, which is particularly concerning for diabetic patients.
Long-Term Side Effects: Chronic use of prednisolone can lead to a constellation of symptoms known as iatrogenic Cushing's syndrome. This includes the redistribution of body fat (resulting in a "moon face" and a "buffalo hump" on the back of the neck), thinning of the skin, easy bruising, and poor wound healing.
Severe Systemic Risks:
- Osteoporosis: Prednisolone inhibits bone formation and increases bone resorption, leading to a rapid loss of bone density and a high risk of fractures, particularly in the spine and ribs.
- Immunosuppression: By suppressing the immune system, it makes patients highly susceptible to infections, including opportunistic infections that would not normally affect a healthy person. It can also mask the signs of an infection until it becomes severe.
- Ocular Effects: Long-term use significantly increases the risk of developing posterior subcapsular cataracts and glaucoma.
- Cardiovascular and Metabolic: It can cause hypertension (due to fluid retention), dyslipidemia, and steroid-induced diabetes mellitus.
The Critical Importance of Tapering
One of the most dangerous mistakes a patient can make is abruptly stopping prednisolone after taking it for more than a few weeks. This can lead to a potentially fatal condition known as acute adrenal crisis.
HPA Axis Suppression: The body's natural production of cortisol is regulated by the hypothalamic-pituitary-adrenal (HPA) axis. When a patient takes exogenous corticosteroids like prednisolone, the brain senses the high levels of steroids in the blood and signals the adrenal glands to stop producing natural cortisol. Over time, the adrenal glands atrophy (shrink) and go dormant.
The Tapering Protocol: If the medication is stopped suddenly, the dormant adrenal glands cannot immediately resume cortisol production. The body is left without this essential hormone, leading to severe fatigue, weakness, nausea, vomiting, dangerous drops in blood pressure, and potentially shock and death. To prevent this, the dose of prednisolone must be gradually reduced (tapered) over weeks or months. This slow reduction gives the HPA axis time to "wake up" and for the adrenal glands to resume their normal, life-sustaining function.
Available Dosages and Administration Guidelines
Prednisolone is available in various formulations, including oral tablets, orally disintegrating tablets (ODT), liquid solutions, syrups, and eye drops. The dosage is highly individualized based on the disease being treated and the patient's response.
Low to Moderate Dosing (5mg - 20mg)
Low doses are typically used for maintenance therapy in chronic autoimmune conditions like rheumatoid arthritis or lupus, after the acute flare-up has been controlled. The goal is to use the lowest possible dose that keeps symptoms at bay to minimize long-term side effects. It is usually taken once daily in the morning to mimic the body's natural cortisol rhythm.
High Dosing (40mg - 60mg+)
High doses are reserved for acute, severe inflammatory crises, such as severe asthma attacks, acute exacerbations of MS, or severe allergic reactions. This high dose is usually maintained for a short period (e.g., 3 to 10 days) to rapidly suppress the immune response, followed by a strict tapering schedule.
Alternate-Day Therapy (ADT)
To minimize the suppression of the HPA axis and reduce long-term side effects, doctors sometimes prescribe alternate-day therapy. In this regimen, the patient takes double the daily dose every other morning. This allows the adrenal glands to recover slightly on the "off" days. ADT is particularly useful for patients requiring long-term maintenance therapy, though it is not suitable for all conditions.
Generic vs. Brand Name Prednisolone
Prednisolone has been available for decades and is widely prescribed as a low-cost generic medication. However, several brand-name formulations exist, often designed for specific patient populations or delivery methods.
Generic Prednisolone: Available as tablets and liquid solutions, generic prednisolone is bioequivalent to the brand names and is the standard of care for most patients due to its affordability and efficacy.
Brand Name Formulations:
- Orapred / Orapred ODT: These are orally disintegrating tablets that dissolve on the tongue without water. They are particularly useful for children who cannot swallow pills or patients with severe nausea.
- Pediapred: A liquid oral solution specifically formulated and flavored for pediatric use, allowing for precise, weight-based dosing in children.
- Millipred: Another oral solution formulation, often preferred for its specific concentration and flavor profile.
- Omnipred: Available as both tablets and oral solution.
The choice between generic and brand-name formulations usually comes down to patient preference (e.g., the need for a liquid or ODT form), insurance coverage, and the specific concentration required for accurate dosing.
Purchasing Prednisolone: Cost, Insurance, and Legal Acquisition
Prednisolone is a potent prescription medication and cannot be legally purchased over-the-counter in the United States or most other developed nations.
Cost and Insurance: Generic prednisolone tablets are extremely inexpensive, often costing less than $10 for a standard short-term course. Liquid formulations (like generic Pediapred) are slightly more expensive but are still highly affordable. It is covered by virtually all Medicare, Medicaid, and commercial insurance plans as a Tier 1 generic. Brand-name ODT formulations (like Orapred) can be significantly more expensive and may require prior authorization.
Legal Acquisition: Obtaining prednisolone requires a valid prescription from a licensed healthcare provider following a medical evaluation. Because of the severe risks associated with improper use (such as adrenal crisis or severe immunosuppression), it is critical that patients only use prednisolone under strict medical supervision.
Counterfeit Warning: Patients should never attempt to purchase prednisolone from unverified online sources or overseas pharmacies that do not require a prescription. The risks of receiving counterfeit, contaminated, or incorrectly dosed medication are high, and the consequences of mismanaging steroid therapy can be fatal.
Drug Interactions: A Comprehensive Overview
Prednisolone interacts with a wide variety of other medications, which can either alter the effectiveness of the steroid or increase the risk of severe side effects.
NSAIDs and GI Bleeding: Combining prednisolone with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) like ibuprofen, naproxen, or aspirin significantly increases the risk of severe gastrointestinal ulceration and bleeding. Both classes of drugs irritate the stomach lining, and their combined effect is synergistic.
Antidiabetic Medications: Because prednisolone raises blood glucose levels by promoting gluconeogenesis in the liver and increasing insulin resistance, patients taking insulin or oral antidiabetic drugs will likely need their dosages adjusted upward while on steroid therapy to maintain glycemic control.
CYP3A4 Inducers and Inhibitors: Prednisolone is metabolized in the liver by the cytochrome P450 3A4 (CYP3A4) enzyme. Drugs that induce this enzyme (like rifampin, phenytoin, and phenobarbital) will clear prednisolone from the body faster, requiring a higher dose of the steroid. Conversely, drugs that inhibit CYP3A4 (like ketoconazole, erythromycin, and certain HIV protease inhibitors) will cause prednisolone to accumulate in the blood, increasing the risk of toxicity.
Live Vaccines: Patients taking immunosuppressive doses of prednisolone must not receive live attenuated vaccines (such as the MMR, yellow fever, or oral polio vaccines). Because their immune system is suppressed, the weakened virus in the vaccine can replicate unchecked, causing a severe or even fatal infection.
Prednisolone Use in Children and Adolescents
The use of systemic corticosteroids in pediatric patients requires extreme caution and specialized monitoring due to the unique risks posed to growing bodies.
Growth Suppression: The most significant concern with long-term prednisolone use in children is the suppression of linear growth. Corticosteroids inhibit the release of growth hormone and directly impair the formation of new bone and cartilage at the epiphyseal plates (growth plates). Even relatively low doses, if given chronically, can result in a child failing to reach their genetically predetermined adult height.
Mitigation Strategies: To minimize this risk, pediatricians strive to use the lowest effective dose for the shortest possible time. When long-term therapy is unavoidable (such as in severe asthma or nephrotic syndrome), alternate-day therapy (ADT) is heavily favored, as it has been shown to cause significantly less growth suppression than daily dosing. Regular monitoring of height and weight on standardized growth charts is mandatory for any child on chronic steroid therapy.
Prednisolone in Elderly Patients
Geriatric patients are particularly vulnerable to the adverse effects of prednisolone, and its use in this population requires careful risk-benefit analysis.
Osteoporosis and Fractures: Older adults, particularly postmenopausal women, already have a higher baseline risk of osteoporosis. Prednisolone rapidly accelerates bone loss, making vertebral compression fractures and hip fractures a major concern. Prophylactic treatment with bisphosphonates, calcium, and vitamin D is often initiated concurrently with long-term steroid therapy in this demographic.
Cognitive and Psychiatric Effects: Elderly patients are more susceptible to steroid-induced psychiatric side effects, including severe mood swings, insomnia, and a condition known as "steroid psychosis," which can manifest as delirium, hallucinations, or severe depression. Furthermore, the fluid retention caused by prednisolone can exacerbate underlying congestive heart failure or hypertension, which are common in older populations.
Dietary Considerations While on Prednisolone
Diet plays a crucial role in mitigating the side effects of prednisolone, particularly during long-term therapy.
Sodium and Fluid Retention: Prednisolone causes the kidneys to retain sodium and excrete potassium. This leads to fluid retention, swelling, and increased blood pressure. Patients are strongly advised to adopt a low-sodium diet, avoiding processed foods, canned soups, and excessive table salt.
Potassium and Calcium: To counteract the loss of potassium, patients should increase their intake of potassium-rich foods like bananas, spinach, and sweet potatoes. Because prednisolone impairs calcium absorption in the gut and increases its excretion in the urine, a diet high in calcium and vitamin D (or appropriate supplementation) is essential to protect bone health.
Protein and Blood Sugar: Steroids cause muscle wasting (myopathy) by breaking down proteins. A high-protein diet can help counteract this effect. Additionally, because prednisolone spikes blood sugar levels, patients should limit their intake of simple carbohydrates and refined sugars to prevent steroid-induced diabetes.
The History of Corticosteroids
The development of corticosteroids is one of the most significant milestones in modern medical history, fundamentally changing the treatment of inflammatory diseases.
The Nobel Prize of 1950: The story began in the 1930s and 40s when researchers Philip Hench, Edward Kendall, and Tadeus Reichstein isolated and synthesized cortisone from the adrenal glands. In 1948, Hench administered the newly synthesized cortisone to a patient crippled by rheumatoid arthritis. The results were miraculous; within days, the bedridden patient was walking. This groundbreaking discovery earned Hench, Kendall, and Reichstein the Nobel Prize in Physiology or Medicine in 1950.
The Creation of Prednisolone: While cortisone was a miracle drug, it had severe side effects, particularly massive fluid retention. In the early 1950s, chemists at the Schering Corporation sought to create a synthetic version that was more potent against inflammation but caused less salt and water retention. By introducing a double bond into the chemical structure of cortisol, they created prednisone and its active metabolite, prednisolone, which were introduced to the market in 1955. These synthetic derivatives proved to be 4 to 5 times more potent than natural cortisol, solidifying their place as essential medicines.
Government and Regulatory Resources
For the most accurate, up-to-date, and comprehensive information regarding prednisolone, patients and healthcare professionals should consult official government and regulatory resources:
- U.S. Food and Drug Administration (FDA): The FDA provides access to the official prescribing information, safety alerts, and guidelines for all approved formulations of prednisolone. (fda.gov)
- National Institutes of Health (NIH) / DailyMed: DailyMed, provided by the National Library of Medicine, offers the most recent, comprehensive package inserts and labeling information submitted to the FDA. (dailymed.nlm.nih.gov)
- National Center for Biotechnology Information (NCBI): The NCBI's StatPearls database provides peer-reviewed, clinical overviews of prednisolone's pharmacology, indications, and adverse effects. (ncbi.nlm.nih.gov)
- World Health Organization (WHO): The WHO includes prednisolone on its Model List of Essential Medicines, highlighting its critical importance in global public health. (who.int)
Prednisolone in Veterinary Medicine
Prednisolone is not only a cornerstone of human medicine but also an indispensable tool in veterinary pharmacology, particularly for the treatment of companion animals like dogs and cats.
The Feline Hepatic Limitation: As previously discussed, the distinction between prednisone and prednisolone is critical in veterinary medicine. Cats have a significantly lower capacity for hepatic biotransformation compared to dogs or humans. They lack sufficient levels of the enzyme required to efficiently convert the prodrug prednisone into the active prednisolone. Therefore, when treating feline patients for inflammatory or immune-mediated conditions, veterinarians must prescribe prednisolone directly to ensure therapeutic efficacy.
Common Veterinary Indications: In dogs and cats, prednisolone is frequently used to manage severe allergic reactions (such as flea allergy dermatitis or atopy), immune-mediated hemolytic anemia (IMHA), inflammatory bowel disease (IBD), and asthma (particularly in cats). It is also used as part of palliative care or chemotherapy protocols for certain veterinary cancers, such as lymphoma.
Veterinary Side Effects: Animals experience side effects similar to humans, including increased thirst (polydipsia), increased urination (polyuria), and increased appetite (polyphagia). Long-term use in dogs can lead to iatrogenic hyperadrenocorticism (Cushing's disease), characterized by a pot-bellied appearance, hair loss, and panting. Cats are generally more resistant to the side effects of corticosteroids than dogs, but long-term use can still induce diabetes mellitus or congestive heart failure in susceptible felines.
Managing the Psychological and Emotional Impact
While the physical side effects of prednisolone are well-documented, the psychological and emotional impacts are often under-discussed, yet they can be profoundly distressing for patients.
The Spectrum of Mood Changes: Corticosteroids can induce a wide range of psychiatric symptoms. In the short term, many patients experience a mild euphoria or a feeling of being "wired" or overly energetic, often accompanied by insomnia. However, this can quickly shift to irritability, severe anxiety, emotional lability (rapid mood swings), and crying spells.
Steroid Psychosis: In rare cases, particularly with high doses (e.g., greater than 40mg per day), patients can develop "steroid psychosis." This is a severe psychiatric emergency characterized by delirium, severe depression, mania, or frank hallucinations and delusions. It typically occurs within the first few weeks of therapy.
Coping Strategies: Patients and their families must be educated about these potential mood changes before starting therapy. If severe psychiatric symptoms occur, the prescribing physician must be notified immediately. Management may involve lowering the steroid dose, switching to an alternate-day regimen, or, in severe cases, prescribing psychotropic medications (such as antipsychotics or mood stabilizers) until the steroid course is completed.
Prednisolone and Pregnancy: Risks and Considerations
The use of prednisolone during pregnancy requires a careful balancing act between controlling the mother's underlying disease and protecting the developing fetus.
Placental Transfer and Metabolism: Prednisolone does cross the placenta, but the placenta contains an enzyme (11-beta-hydroxysteroid dehydrogenase type 2) that actively metabolizes prednisolone back into the inactive prednisone, protecting the fetus from high levels of active steroid. Because of this placental barrier, prednisolone is often preferred over other steroids (like dexamethasone or betamethasone, which cross the placenta more readily) when treating maternal conditions during pregnancy.
Fetal Risks: Despite this placental protection, systemic corticosteroid use during the first trimester has been associated with a slightly increased risk of oral clefts (cleft lip or palate) in the fetus. Use later in pregnancy can increase the risk of intrauterine growth restriction (IUGR), premature rupture of membranes, and low birth weight. Furthermore, if the mother receives high doses near the time of delivery, the newborn must be carefully monitored for signs of adrenal suppression (hypoadrenalism).
The Clinical Decision: Ultimately, uncontrolled severe maternal disease (such as a severe asthma attack or a lupus flare) poses a much greater risk to both the mother and the fetus than the medication itself. Therefore, prednisolone is used during pregnancy when the benefits clearly outweigh the risks, typically at the lowest effective dose.
Lifestyle Modifications and Supportive Care
Patients on long-term prednisolone therapy must adopt specific lifestyle modifications to counteract the drug's systemic effects and maintain their overall health.
Exercise and Muscle Health: Because prednisolone causes muscle wasting (steroid myopathy) and bone loss, a consistent exercise regimen is vital. Weight-bearing exercises (like walking or light resistance training) help stimulate bone formation and maintain muscle mass. However, patients with severe joint inflammation (e.g., active rheumatoid arthritis) must balance exercise with adequate rest to avoid joint damage.
Infection Prevention: Due to the immunosuppressive nature of the drug, patients must be vigilant about hygiene. This includes frequent handwashing, avoiding crowds during flu season, and staying away from individuals who are visibly ill. As mentioned earlier, they must also ensure their vaccinations (non-live) are up to date, ideally before starting long-term therapy.
Skin Care: Prednisolone thins the skin, making it fragile, prone to bruising, and slow to heal. Patients should use gentle, fragrance-free moisturizers to maintain the skin barrier, avoid harsh soaps, and protect their skin from trauma and excessive sun exposure.
Sleep Hygiene: Steroid-induced insomnia is a common complaint. Patients should practice strict sleep hygiene, such as maintaining a cool, dark bedroom, avoiding screens before bed, and establishing a consistent sleep schedule. If the medication is taken once daily, taking it early in the morning can help minimize its impact on nighttime sleep.
Prednisolone in the Treatment of Inflammatory Bowel Disease (IBD)
Inflammatory Bowel Disease (IBD), which primarily encompasses Crohn's disease and ulcerative colitis, involves chronic, severe inflammation of the gastrointestinal tract. Prednisolone plays a critical, albeit temporary, role in the management of these debilitating conditions.
Inducing Remission: During acute flare-ups of IBD, patients experience severe abdominal pain, bloody diarrhea, weight loss, and profound fatigue. In these acute crises, systemic corticosteroids like prednisolone are the most effective agents for rapidly suppressing the intense mucosal inflammation and inducing clinical remission. They work much faster than immunomodulators (like azathioprine) or biologic therapies (like infliximab), which can take weeks or months to reach full efficacy.
The Bridge Therapy Concept: It is crucial to understand that prednisolone is used as a "bridge" therapy in IBD, not a maintenance therapy. Because of the severe long-term side effects (osteoporosis, diabetes, infection risk), the goal is to use prednisolone to quickly calm the flare-up while simultaneously starting a safer, long-term maintenance medication. Once the maintenance drug begins to work, the prednisolone is carefully tapered off.
Steroid Dependency and Resistance: A significant challenge in IBD management is that some patients become "steroid-dependent," meaning their symptoms return every time the prednisolone dose is lowered, making it impossible to taper off completely. Others become "steroid-resistant," where the medication fails to induce remission even at high doses. In both scenarios, gastroenterologists must quickly pivot to alternative therapies, such as biologics or, in severe cases, surgical intervention (such as bowel resection).
The Impact of Prednisolone on the Endocrine System
Because prednisolone is a synthetic hormone, its introduction into the body profoundly disrupts the normal functioning of the endocrine system, leading to widespread metabolic consequences.
Steroid-Induced Diabetes Mellitus: One of the most common and serious metabolic side effects is the development of steroid-induced diabetes. Prednisolone increases blood glucose levels through two primary mechanisms: it stimulates the liver to produce more glucose (gluconeogenesis), and it causes the body's tissues (especially muscle and fat) to become resistant to insulin. Patients with pre-existing diabetes will almost certainly require increased doses of insulin or oral hypoglycemic agents. Even patients without a history of diabetes can develop significant hyperglycemia, requiring close monitoring of blood sugar levels and potentially the temporary initiation of insulin therapy.
Thyroid Function Alterations: High doses of corticosteroids can suppress the secretion of Thyroid Stimulating Hormone (TSH) from the pituitary gland. While this rarely causes overt clinical hypothyroidism, it can complicate the interpretation of thyroid function tests, making it difficult to accurately diagnose underlying thyroid disorders while the patient is on steroid therapy.
Lipid Metabolism and Fat Redistribution: Prednisolone alters lipid metabolism, frequently leading to elevated levels of triglycerides and LDL ("bad") cholesterol, increasing the long-term risk of cardiovascular disease. Furthermore, it causes a characteristic redistribution of body fat. Fat is lost from the extremities (arms and legs) and deposited centrally, leading to the classic "moon face" (facial rounding), "buffalo hump" (dorsocervical fat pad), and truncal obesity associated with Cushing's syndrome.
Ophthalmic Applications: Prednisolone Eye Drops
While systemic (oral or intravenous) prednisolone affects the entire body, localized formulations are used to treat specific areas while minimizing systemic side effects. Prednisolone acetate ophthalmic suspension (eye drops) is a prime example.
Treating Ocular Inflammation: Prednisolone eye drops are highly effective in treating severe, non-infectious inflammation of the eye. This includes conditions like uveitis (inflammation of the middle layer of the eye), iritis, severe allergic conjunctivitis, and inflammation following ocular surgery (such as cataract removal or corneal transplants). By applying the steroid directly to the surface of the eye, high local concentrations are achieved, rapidly reducing redness, pain, and swelling.
The Risk of Glaucoma and Cataracts: Even when applied topically, prednisolone carries significant risks for the eye. Prolonged use of steroid eye drops can cause a dangerous increase in intraocular pressure (IOP), leading to steroid-induced glaucoma and potential damage to the optic nerve. It also significantly accelerates the formation of posterior subcapsular cataracts. Therefore, patients using prednisolone eye drops must be closely monitored by an ophthalmologist, with frequent checks of their intraocular pressure and lens clarity.
Contraindication in Viral Infections: It is absolutely critical that prednisolone eye drops are never used to treat a "red eye" without a proper medical diagnosis. If the redness is caused by a viral infection, particularly Herpes simplex keratitis, applying a steroid will suppress the local immune response, allowing the virus to replicate wildly. This can lead to severe corneal ulceration, scarring, and permanent blindness.
Prednisolone Quick View
| Active Ingredient | Prednisolone |
|---|---|
| Manufacturer | Various Generics / Concordia (Orapred) |
| Type | Glucocorticoid (Corticosteroid) |
| Onset | Rapid (1-2 hours for oral, immediate for IV) |
| Duration | 12-36 hours (Biological half-life) |
| Food Interaction | Take with food or milk to prevent severe stomach upset and ulceration. |
| Alcohol | Avoid; alcohol significantly increases the risk of severe gastrointestinal bleeding and ulcers. |
| Prescription | Required (Strict Medical Supervision) |
Prednisolone Side Effects
Common Side Effects
- Increased appetite and weight gain.
- Fluid retention (swelling in face and ankles).
- Insomnia and restlessness.
- Mood swings, irritability, or mild euphoria.
- Elevated blood sugar levels.
Uncommon Side Effects
- Redistribution of body fat (moon face, buffalo hump).
- Thinning of the skin and easy bruising.
- Muscle weakness (steroid myopathy).
- Increased susceptibility to infections.
- Severe anxiety or depression.
Rare Side Effects
- Steroid psychosis (delirium, hallucinations).
- Osteoporosis and compression fractures.
- Glaucoma and posterior subcapsular cataracts.
- Avascular necrosis of the femoral head.
- Peptic ulcer disease and GI bleeding.
Important Warning: BLACK BOX WARNING: Abrupt discontinuation after long-term use can cause fatal acute adrenal crisis. MUST taper dose slowly under medical supervision.
More Information About Prednisolone
Storage
Store at controlled room temperature (15°C to 30°C / 59°F to 86°F). Protect from heat, light, and excessive moisture. Keep liquid formulations tightly closed.
Contraindications
Prednisolone is strictly contraindicated in: 1. Systemic fungal infections. 2. Known hypersensitivity to prednisolone. 3. Administration of live or live-attenuated vaccines (in patients receiving immunosuppressive doses). 4. Herpes simplex keratitis (for ophthalmic use).
Drug Interactions
Severe interactions with NSAIDs (increased GI bleeding risk), antidiabetic drugs (decreased efficacy), CYP3A4 inducers/inhibitors, and potassium-depleting diuretics.
Prednisolone FAQs
Prednisone is a prodrug that must be converted by the liver into prednisolone to become active. Prednisolone is already active. If you have severe liver disease, you must take prednisolone directly because your liver cannot process prednisone efficiently.
Taking steroids tells your adrenal glands to stop making natural cortisol. If you stop the medication suddenly, your body has no cortisol, leading to a potentially fatal condition called adrenal crisis. Tapering gives your adrenal glands time to wake up and start working again.
No. Combining prednisolone with NSAIDs like ibuprofen, naproxen, or aspirin severely increases your risk of developing stomach ulcers and dangerous gastrointestinal bleeding. Use acetaminophen (Tylenol) for pain instead, after consulting your doctor.
This is a common side effect called 'moon face,' caused by fluid retention and a redistribution of body fat. It typically occurs with long-term use or high doses. It is reversible and will gradually go away after the medication is tapered off.
Written and Reviewed by Our Qualified Team

Find out more about our medical content authors and how we ensure the accuracy of our content.
Content last updated: 21 May 2026
Prednisolone Reviews
Based on 39 reviews
"I've found Prednisolone to be a solid help for those times my condition acts up. It does a good job of taking the edge off and getting me through the worst of it, which is exactly what I need."
I've had Prednisolone a few times for different issues, and it always seems to do the trick in reducing swelling and discomfort. It's pretty straightforward to take and usually kicks in fairly quickly, which is a big plus when you're feeling miserable.
Prednisolone has been a reliable ally in getting my symptoms under control when things get tough. I appreciate how it helps to calm things down, giving me some much-needed relief.
Prednisolone has been a good option for me when I need to get a handle on my symptoms. It's relatively easy to manage and usually helps me feel more comfortable pretty quickly, which is a big plus.
Prednisolone has been a lifesaver for my severe asthma attacks. It really helps to open up my airways and allows me to breathe much easier, which is incredibly reassuring during those scary moments.
Prednisolone has been a lifesaver for me when my asthma acts up. It really helps calm things down quickly so I can breathe easier, which is such a relief.
This medication has been a reliable friend when inflammation flares up. It does a good job of dialing down the discomfort, allowing me to get back to my routine without too much interruption. I find it to be quite predictable in its effects, which is reassuring.
Prednisolone has been a surprisingly effective tool for those stubborn inflammatory moments. It really helps quiet things down when my body decides to act up, and I appreciate how quickly it seems to get to work.
Prednisolone has been a consistent performer for me when my symptoms decide to act up. It's quite easy to integrate into my daily schedule, and I've consistently found it helps dial down the discomfort.
Prednisolone has been a good ally when my immune system gets a bit overzealous. It's easy to take, and I've noticed it really helps to calm things down so I can feel more like myself again.
Prednisolone has been a solid choice for managing my chronic condition. It consistently helps to keep my symptoms in check, making daily life much more comfortable without any fuss.
Prednisolone has been a consistent performer for me. It really helps quiet down my body's overreactions, letting me get on with my day feeling much better.
Prednisolone has been a good ally in calming down my system when it acts up. It's pretty easy to take, and I've noticed a definite improvement in my overall comfort levels when I'm on it.
Prednisolone really helps me manage my persistent inflammation. It’s a straightforward medication to incorporate into my routine, and I definitely feel a sense of relief once it kicks in.
I've found Prednisolone to be quite effective for those times my condition acts up. It's easy enough to take, and I appreciate how it helps calm things down so I can get on with my day.
Prednisolone has been a good ally for calming down my body when it decides to overreact. I appreciate how it helps bring things back to a more manageable level, making daily life a bit smoother.
Prednisolone has been a lifesaver for those difficult flare-ups. It helps me get back on track quicker, and I appreciate how reliably it works.
Prednisolone has been a solid choice for managing my condition. It consistently helps to reduce inflammation and discomfort, allowing me to feel more like myself again without a lot of hassle.
Prednisolone has been a reliable companion for me. It consistently helps to quiet down the overreactions my body sometimes has, making a real difference in how I feel day-to-day.
Prednisolone has been a blessing when my body decides to act up. It really helps take the edge off my symptoms, letting me get on with things without too much fuss.
Prednisolone does a good job of getting things under control when my system feels like it's spinning out. It's easy enough to take, and I notice a definite improvement in how I'm feeling within a day or two.
When my body decides to throw a tantrum, Prednisolone usually steps in and calms the storm. It's not a cure-all, but it reliably dials down the inflammation, making a real difference in my comfort levels. It’s a relief to have something that can bring things back to a more tolerable state.
Prednisolone has been a lifesaver for me when things get really bad. It consistently helps reduce the swelling and pain, allowing me to get some much-needed relief and function a bit more normally. I'm grateful to have it as an option.
Prednisolone often feels like hitting a reset button for my system when things get out of whack. It typically brings down the inflammation pretty quickly, allowing me to get back to feeling more like myself.
Prednisolone has been a consistent helper for me when things get inflamed. It reliably reduces that uncomfortable feeling, allowing me to get on with my day much easier.
Prednisolone has been a consistent performer for me when my symptoms get out of hand. It really helps calm things down and makes a noticeable difference in how I feel, allowing me to get back to my daily activities more comfortably.
This medication has been quite effective in getting my body back on track when things flare up. I appreciate how quickly it seems to work, making a noticeable difference in my comfort levels.
Prednisolone has been a real game-changer for me when my inflammation acts up. It's surprisingly easy to take, and I usually start feeling the benefits within a day or two, which is a huge relief.
Prednisolone has been a solid choice for those times my body just needs a little extra nudge to get things under control. It really helps to settle things down and lets me get back to feeling more like myself without a lot of fuss.
Prednisolone has been a real game-changer for getting my symptoms under control when they flare up. It works pretty quickly to reduce the discomfort, which is a huge relief when you're not feeling your best.
"Prednisolone has been a reliable part of my treatment plan. It consistently helps calm down flare-ups, allowing me to get back to my routine without too much disruption."
Taking Prednisolone has generally been a smooth experience for me. It does a good job of taking the edge off my symptoms, making day-to-day life much more manageable when things flare up.
This medication has been a lifesaver for those times my condition flares up, helping to bring things back to a manageable level. I'm always impressed by how quickly it seems to get to work, which is a huge relief.
Prednisolone has been a real game-changer for those days my symptoms decide to act up. It helps me feel much more like myself again, allowing me to get back to my routine without too much fuss.
Prednisolone has been a real game-changer for me when my symptoms flare up. It helps settle things down quite quickly, allowing me to get back to feeling more normal without too much fuss.
Prednisolone has been a steady hand when my body needs a bit of a reset. It's been pretty straightforward to take and generally helps me feel more settled when things are flaring up.
Prednisolone has been a good ally when my body acts up with inflammation. It really helps calm things down so I can get back to feeling more like myself. I'm grateful for how it helps bring things back to normal.
Prednisolone has been a steady companion for me when my symptoms act up. It consistently helps calm things down, making those difficult periods much more manageable without too much drama.
I've found Prednisolone to be quite useful for those times when my body just needs a little reset. It really helps calm things down and lets me get back to feeling more comfortable.
Leave a Review
How Does It Work?
Research
Read our comprehensive review to understand the medication
Consult Your Doctor
Discuss the medication with your healthcare provider
Get Your Prescription
Obtain a valid prescription from your doctor