
Clomid (Clomid)
Women's Health Treatment
The definitive medical guide to Clomid (clomiphene citrate): clinical applications, safety protocols, legal acquisition, and comprehensive patient education.
Table of Contents
Clomid Product Information
What is Clomid / Clomiphene Citrate?
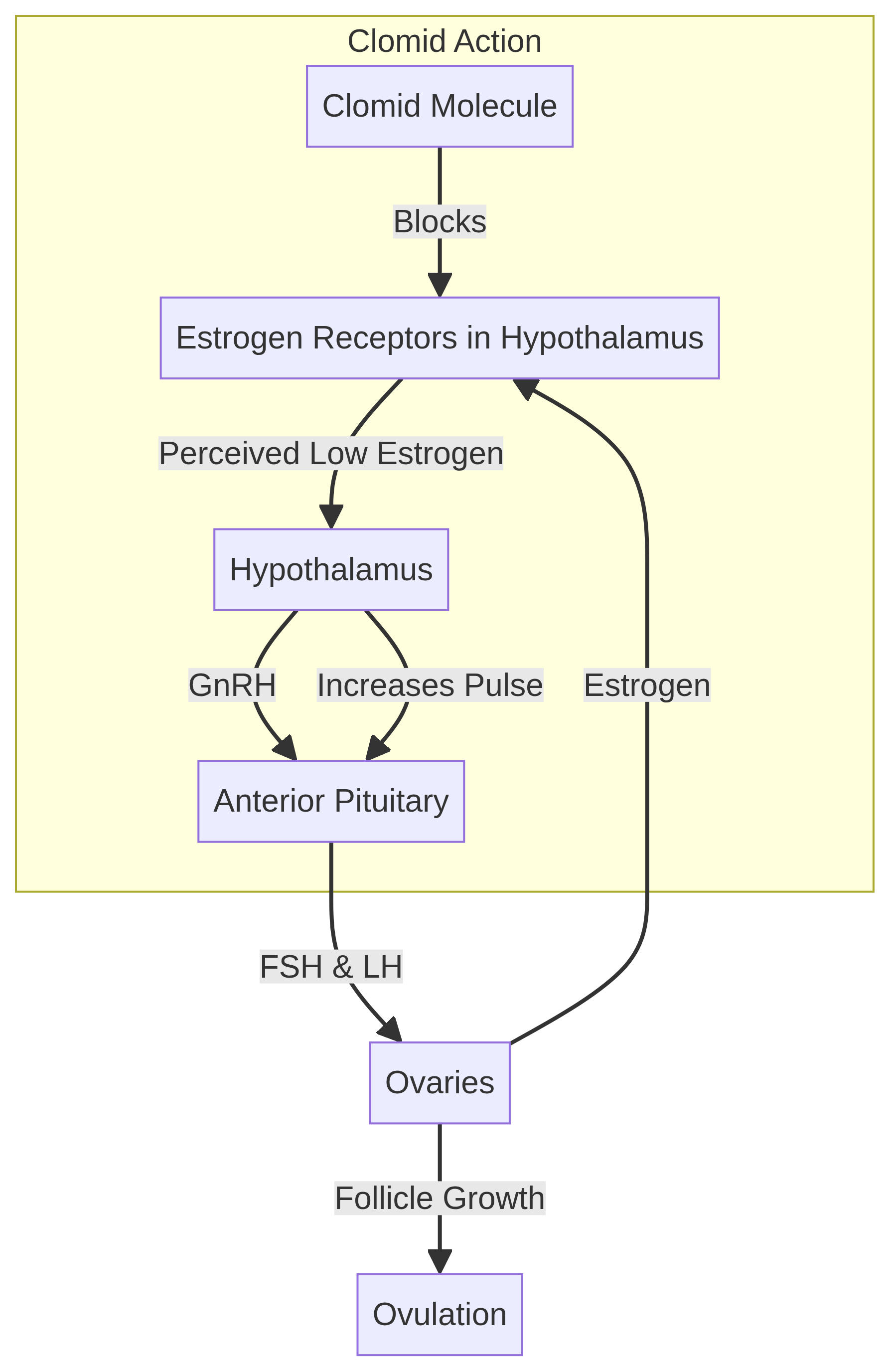
Clomiphene citrate, commercially known as Clomid, is a non-steroidal medication that belongs to a class of drugs called Selective Estrogen Receptor Modulators (SERMs). It has been the cornerstone of reproductive medicine since its FDA approval in 1967. Unlike direct hormonal injections, Clomid acts 'upstream' by modulating the body's natural endocrine feedback loops. It is primarily used to induce ovulation in women who have difficulty conceiving due to irregular or absent menstrual cycles. By binding to estrogen receptors in the hypothalamus, Clomid 'tricks' the brain into perceiving a state of low estrogen, which in turn triggers the release of the hormones necessary for follicular development and egg release.
The mechanism of action of clomiphene citrate is fascinating and complex. The hypothalamus, a small region at the base of the brain, acts as the control center for the reproductive system. It releases Gonadotropin-Releasing Hormone (GnRH) in a pulsatile manner, which then stimulates the pituitary gland to produce Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH). These hormones travel to the ovaries, prompting the development of ovarian follicles, each containing an egg. As the follicles grow, they produce estrogen. Normally, rising estrogen levels send a negative feedback signal to the hypothalamus, telling it to slow down GnRH production. Clomid blocks these estrogen receptors, preventing the hypothalamus from sensing the rising estrogen. Consequently, the hypothalamus continues to secrete GnRH, leading to sustained FSH and LH production, which robustly stimulates the ovaries to mature and release an egg.
Clomid is administered orally, typically in the form of a 50mg tablet. It is a mixture of two geometric isomers: enclomiphene and zuclomiphene. Enclomiphene is the more potent anti-estrogenic isomer and is cleared from the body relatively quickly, usually within a few days. Zuclomiphene, on the other hand, has mild estrogenic properties and a much longer half-life, meaning it can remain in the body for weeks or even months after administration. This prolonged presence of zuclomiphene is thought to contribute to some of the sustained effects and potential side effects of the medication.
Over the decades, Clomid has helped millions of women achieve their dream of motherhood. Its oral administration, relatively low cost compared to injectable gonadotropins, and well-understood safety profile make it an attractive first-line option for many fertility specialists. However, it is not a magic pill and requires careful medical supervision to ensure its safe and effective use. Understanding how Clomid works, its potential risks, and the necessary monitoring protocols is essential for anyone embarking on this treatment journey.
FDA-Approved Uses and Clinical Indications
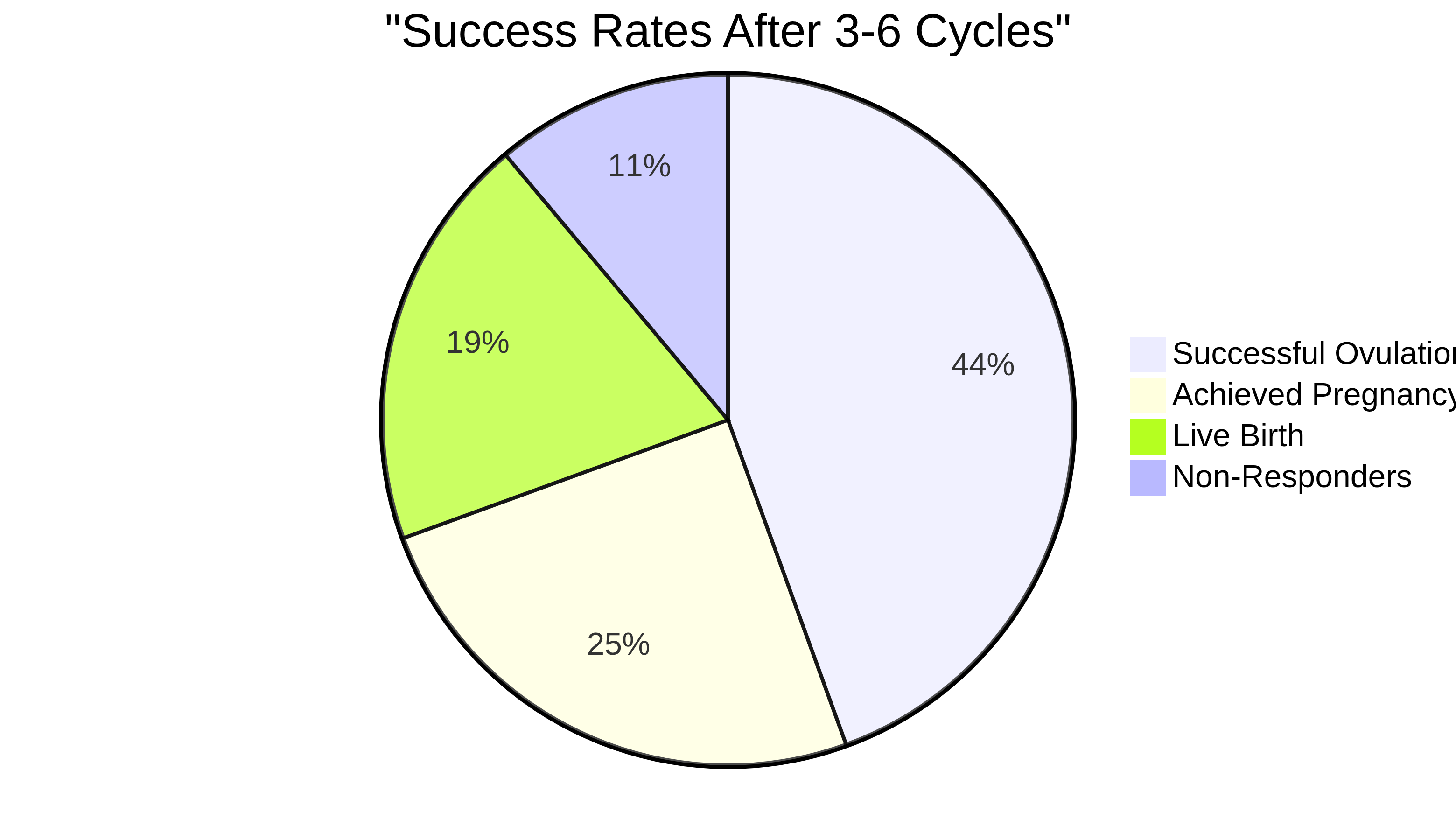
The FDA has approved Clomid specifically for the treatment of ovulatory dysfunction in women who desire pregnancy. This clinical indication covers a range of conditions, most notably Polycystic Ovary Syndrome (PCOS), which is characterized by hormonal imbalances that prevent regular ovulation. Clomid is indicated for patients who have an intact hypothalamic-pituitary-ovarian (HPO) axis and sufficient endogenous estrogen. It is not intended for women whose infertility is caused by primary pituitary or ovarian failure. For many, Clomid is the first pharmacological step in a fertility journey, offering a high success rate for inducing ovulation (approximately 80% within the first three months of use).
Polycystic Ovary Syndrome (PCOS) is one of the most common endocrine disorders in women of reproductive age, affecting up to 10% of this population. Women with PCOS often have elevated levels of androgens (male hormones) and insulin resistance, which disrupt the normal follicular development process. Instead of one follicle maturing and releasing an egg, multiple small follicles develop but fail to mature, leading to anovulation (lack of ovulation) or oligo-ovulation (infrequent ovulation). Clomid's ability to stimulate FSH production helps overcome this developmental arrest, allowing a dominant follicle to emerge and ovulate.
In addition to PCOS, Clomid is also used for women with luteal phase defects. The luteal phase is the second half of the menstrual cycle, following ovulation, during which the corpus luteum produces progesterone to prepare the uterine lining for implantation. If the luteal phase is too short or progesterone levels are inadequate, a fertilized egg may fail to implant, resulting in an early miscarriage. By promoting the development of a robust, healthy follicle, Clomid can indirectly improve the quality of the resulting corpus luteum, thereby enhancing progesterone production and supporting a healthier luteal phase.
Another common indication for Clomid is unexplained infertility. This diagnosis is given when a couple has been trying to conceive for at least a year (or six months if the woman is over 35) without success, and all standard fertility tests—including semen analysis, tubal patency tests, and ovulation confirmation—return normal results. In these cases, Clomid is often prescribed in conjunction with Intrauterine Insemination (IUI). The goal here is not just to induce ovulation, but to induce 'superovulation'—the release of two or three eggs instead of just one. This increases the mathematical probability that at least one egg will meet a healthy sperm and fertilize successfully.
Off-Label Use in Men: A Careful Consideration
Although not FDA-approved for male infertility, Clomid is frequently prescribed 'off-label' by urologists to treat male hypogonadism and idiopathic infertility. In men, the medication works by stimulating the pituitary gland to produce more Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH). LH then signals the testes to produce more natural testosterone, while FSH supports sperm production. This can be a superior alternative to exogenous testosterone therapy, which can actually suppress sperm count. However, this application must be managed with extreme care by a specialist, as incorrect dosing can lead to hormonal imbalances, mood changes, or paradoxical decreases in sperm quality. Regular blood monitoring of testosterone and estradiol levels is essential during male Clomid therapy.
Male hypogonadism is a condition characterized by abnormally low levels of testosterone, which can lead to symptoms such as fatigue, decreased libido, erectile dysfunction, and reduced muscle mass. Traditional testosterone replacement therapy (TRT), while effective for alleviating these symptoms, has a significant drawback for men who wish to maintain their fertility: it suppresses the body's natural production of LH and FSH. Without these hormones, the testes stop producing sperm, leading to severe oligospermia (low sperm count) or azoospermia (absence of sperm). Clomid offers a way to boost testosterone levels while simultaneously supporting, rather than suppressing, spermatogenesis.
The use of Clomid in men is typically considered when the hypogonadism is secondary, meaning the issue lies with the pituitary gland or hypothalamus not sending strong enough signals to the testes, rather than primary testicular failure. By blocking estrogen receptors in the male brain, Clomid increases the pulsatile release of GnRH, which in turn drives up LH and FSH levels. This stimulates the Leydig cells in the testes to produce more testosterone and the Sertoli cells to support sperm maturation.
Despite its benefits, off-label Clomid use in men requires meticulous monitoring. The optimal dosage for men is often lower than that for women, typically ranging from 25mg every other day to 50mg daily. Higher doses do not necessarily yield better results and can lead to an overproduction of estrogen (as excess testosterone is aromatized into estradiol), which can paradoxically suppress the HPG axis and negate the benefits of the treatment. Men taking Clomid may also experience side effects such as mood swings, visual disturbances, and changes in libido. Therefore, treatment should always be overseen by a qualified urologist or reproductive endocrinologist who can regularly assess hormone levels and adjust the dosage as needed.
Who May Be Prescribed Clomid?
Clomid is typically prescribed after a comprehensive fertility workup. Candidates usually include women with PCOS, those with irregular menstrual cycles (oligo-ovulation), or couples diagnosed with 'unexplained infertility.' In the case of unexplained infertility, Clomid is often used to induce 'superovulation'—the release of more than one egg per cycle—to increase the mathematical probability of fertilization. Before a prescription is issued, doctors will ensure that the patient's fallopian tubes are open and that the male partner's sperm count is within a range that makes conception possible. It is not suitable for women with premature ovarian failure or those who are already pregnant.
A thorough fertility evaluation is a prerequisite for Clomid therapy. This evaluation typically begins with a detailed medical history and physical examination. The physician will inquire about menstrual cycle regularity, previous pregnancies, lifestyle factors, and any underlying medical conditions. Blood tests are conducted to assess hormone levels, including Day 3 FSH, LH, estradiol, and Anti-Mullerian Hormone (AMH), which provides an estimate of ovarian reserve. Thyroid function (TSH) and prolactin levels are also checked, as abnormalities in these hormones can interfere with ovulation.
Ensuring tubal patency is a critical step before initiating Clomid. If the fallopian tubes are blocked or damaged, the egg cannot travel from the ovary to the uterus, and sperm cannot reach the egg for fertilization. Tubal patency is usually assessed through a Hysterosalpingogram (HSG), an X-ray procedure in which a contrast dye is injected into the uterus and tubes. If the tubes are blocked, Clomid will not be effective, and alternative treatments, such as In Vitro Fertilization (IVF), must be considered.
Equally important is the evaluation of the male partner. A semen analysis is performed to assess sperm count, motility (movement), and morphology (shape). If the semen parameters are severely abnormal, inducing ovulation in the female partner with Clomid is unlikely to result in pregnancy. In such cases, treatments like Intracytoplasmic Sperm Injection (ICSI) combined with IVF may be necessary. Clomid is most effective when the male partner has normal or only mildly impaired semen parameters.
It is also crucial to identify patients for whom Clomid is not appropriate. Women with primary ovarian insufficiency (premature menopause), where the ovaries have depleted their supply of eggs, will not respond to Clomid. Similarly, women with hypothalamic amenorrhea, a condition often caused by extreme stress, excessive exercise, or low body weight, may not have sufficient endogenous estrogen for Clomid to be effective. In these cases, injectable gonadotropins or lifestyle modifications are more appropriate interventions.
Understanding Side Effects and Serious Risks
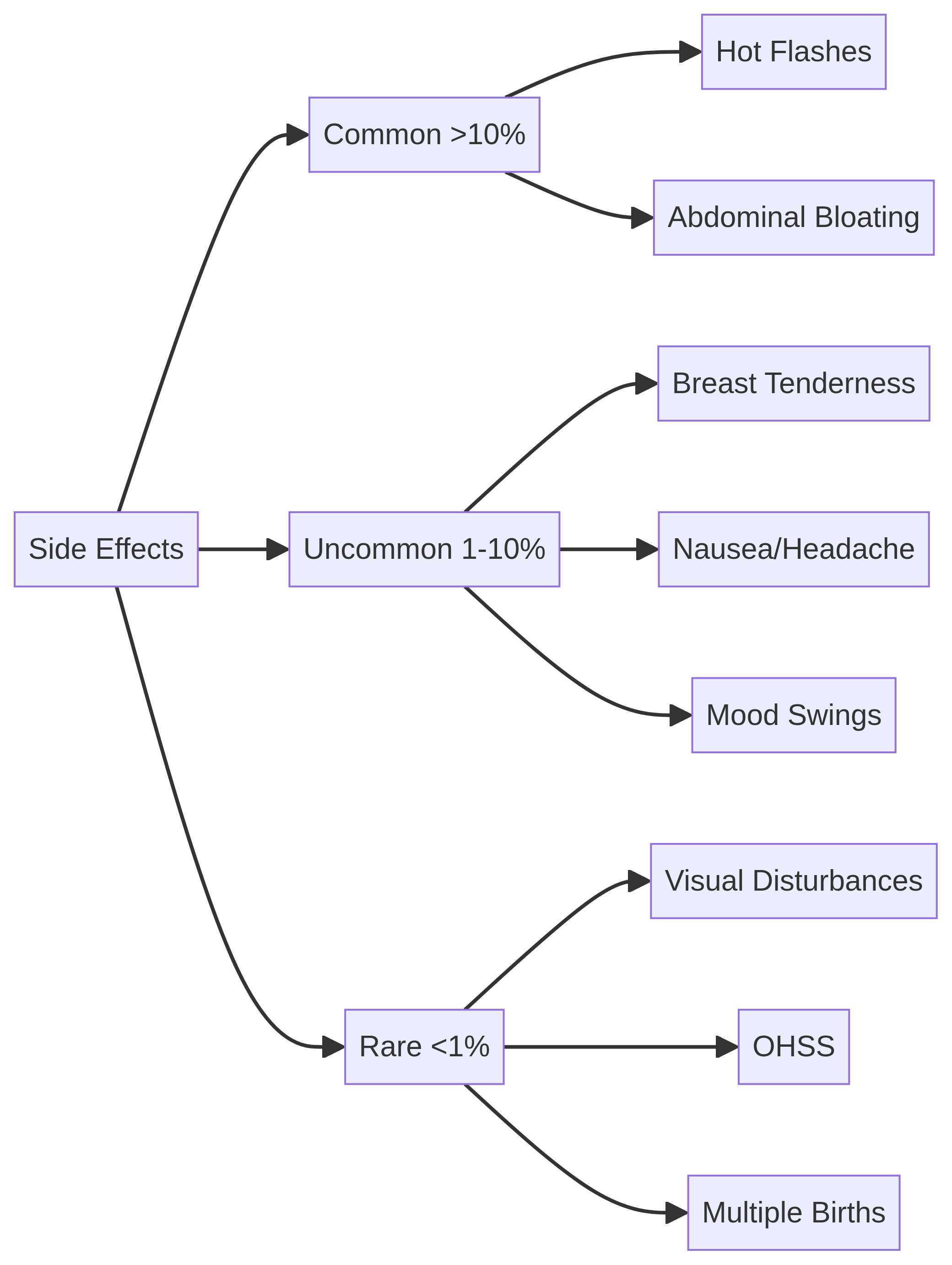
While Clomid is generally well-tolerated, its anti-estrogenic properties can lead to several side effects. Common issues include vasomotor flushes (hot flashes), which affect about 10% of patients, abdominal bloating, breast tenderness, and mood swings—colloquially known as the 'Clomid Crazies.' However, there are three critical risks that every patient must understand:
- Ovarian Hyperstimulation Syndrome (OHSS): This is a serious condition where the ovaries become excessively swollen and leak fluid into the abdomen and chest. While less common with Clomid than with injectable fertility drugs, it is a medical emergency that requires immediate attention.
- Visual Symptoms: Some patients experience blurring, spots, or flashes of light. If any visual changes occur, the medication must be discontinued immediately, as these symptoms can rarely become permanent.
- Multiple Pregnancy: Clomid significantly increases the chance of multiple births. Approximately 5-8% of Clomid pregnancies result in twins, compared to the natural rate of about 1%. Triplets and higher-order multiples occur in less than 1% of cases.
The side effect profile of Clomid is largely driven by its mechanism of action as an estrogen receptor antagonist. By blocking estrogen receptors throughout the body, Clomid can induce symptoms similar to those experienced during menopause. Hot flashes are among the most frequently reported side effects, characterized by sudden feelings of warmth, flushing, and sweating. These episodes are usually transient and subside once the medication is discontinued. Other common estrogen-deprivation symptoms include vaginal dryness, which can interfere with intercourse and sperm transport, and changes in cervical mucus quality, making it less hospitable to sperm.
Mood swings and emotional lability are also widely recognized side effects of Clomid. The hormonal fluctuations induced by the medication can exacerbate underlying anxiety or depression, leading to irritability, tearfulness, and difficulty concentrating. Patients and their partners should be prepared for these potential emotional shifts and maintain open communication with their healthcare provider. In severe cases, the psychological impact may necessitate discontinuing the medication or exploring alternative treatments.
Ovarian Hyperstimulation Syndrome (OHSS) is a rare but potentially life-threatening complication of ovulation induction. It occurs when the ovaries over-respond to the medication, developing numerous large cysts and releasing vasoactive substances that increase capillary permeability. This causes fluid to leak from the blood vessels into the abdominal cavity (ascites) and sometimes the pleural cavity (pleural effusion). Symptoms of OHSS include severe abdominal pain, rapid weight gain, nausea, vomiting, and shortness of breath. Mild cases can be managed with rest and hydration, but severe OHSS requires hospitalization for intravenous fluids, pain management, and sometimes paracentesis to drain the accumulated fluid.
Visual disturbances are another serious, albeit uncommon, side effect of Clomid. Patients may report blurred vision, double vision, scotomata (blind spots), or photopsia (flashes of light). These symptoms are thought to be related to the drug's effect on the optic nerve or visual cortex. Any patient experiencing visual changes while taking Clomid must stop the medication immediately and undergo a thorough ophthalmologic evaluation. In most cases, the symptoms resolve within a few days or weeks after discontinuing the drug, but irreversible visual impairment has been reported in rare instances.
The risk of multiple gestation is a significant consideration when using Clomid. Because the medication stimulates the development of multiple follicles, there is a higher probability that more than one egg will be released and fertilized. While many couples may welcome the idea of twins, multiple pregnancies carry higher risks of complications, including premature birth, low birth weight, gestational diabetes, and preeclampsia. The risk of higher-order multiples (triplets or more) is relatively low with Clomid (less than 1%), but it is still a possibility that must be discussed with the patient prior to initiating treatment.
Contraindications: When Clomid is Not Safe
Clomid is strictly contraindicated in several scenarios. It must never be taken during pregnancy, as it can cause harm to the developing fetus. Other contraindications include active liver disease or a history of liver dysfunction, as the drug is metabolized in the liver. It should not be used if there is undiagnosed abnormal uterine bleeding, as this could mask underlying conditions like endometrial cancer. Furthermore, it is not safe for women with ovarian cysts (unrelated to PCOS) or those with uncontrolled thyroid or adrenal gland disorders. Patients with a known hypersensitivity to clomiphene citrate must also avoid the medication.
The contraindication during pregnancy is absolute. Clomid is classified as a Pregnancy Category X drug by the FDA, meaning that studies in animals or humans have demonstrated fetal abnormalities, and the risks involved in use of the drug in pregnant women clearly outweigh potential benefits. Because Clomid has a long half-life, it is crucial to ensure that a woman is not pregnant before starting a new cycle of treatment. A baseline pregnancy test is often recommended, especially for women with irregular cycles who may not realize they have conceived.
Liver disease is another major contraindication. Clomiphene citrate is extensively metabolized by the liver and excreted primarily in the feces via the biliary tract. In patients with impaired hepatic function, the drug can accumulate to toxic levels, exacerbating liver damage and increasing the risk of severe side effects. A thorough medical history and, if necessary, liver function tests should be conducted before prescribing Clomid to ensure the patient's liver can safely process the medication.
Undiagnosed abnormal uterine bleeding is a red flag that must be investigated before initiating any fertility treatment. Irregular bleeding can be a symptom of various underlying conditions, including endometrial polyps, fibroids, or even endometrial hyperplasia or cancer. Clomid's estrogenic and anti-estrogenic effects can stimulate the endometrial lining, potentially worsening these conditions or masking their symptoms. A definitive diagnosis, often requiring an endometrial biopsy or hysteroscopy, must be established to rule out malignancy or other serious pathology.
The presence of ovarian cysts, other than the small polycystic ovaries characteristic of PCOS, is also a contraindication. Clomid stimulates ovarian follicular growth, which can cause existing cysts to enlarge, potentially leading to cyst rupture or ovarian torsion (twisting of the ovary on its blood supply). Both of these are acute medical emergencies requiring surgical intervention. A baseline transvaginal ultrasound is typically performed before starting Clomid to confirm the absence of significant ovarian cysts.
Finally, uncontrolled thyroid or adrenal dysfunction must be addressed before using Clomid. The thyroid and adrenal glands play crucial roles in regulating metabolism and hormone production. Disorders such as hypothyroidism, hyperthyroidism, or congenital adrenal hyperplasia can disrupt the HPO axis and cause anovulation. Treating these underlying endocrine disorders is often sufficient to restore normal ovulation without the need for Clomid. If Clomid is used in the presence of uncontrolled thyroid or adrenal disease, it is less likely to be effective and may complicate the management of the primary condition.
Available Dosages and Clinical Monitoring
The dosage of Clomid is determined solely by a healthcare provider based on the patient's medical history and response to treatment. It is critical to follow the prescribed protocol exactly; taking more than directed does not increase the chances of pregnancy but does significantly increase the risk of serious side effects. Most doctors will monitor the cycle with transvaginal ultrasounds to track follicle growth and blood tests to confirm ovulation.
Clinical monitoring is a cornerstone of safe and effective Clomid therapy. The goal of monitoring is twofold: to assess the patient's response to the medication and to mitigate the risks of complications such as OHSS and multiple gestation. Monitoring typically involves a combination of transvaginal ultrasounds and serum hormone measurements.
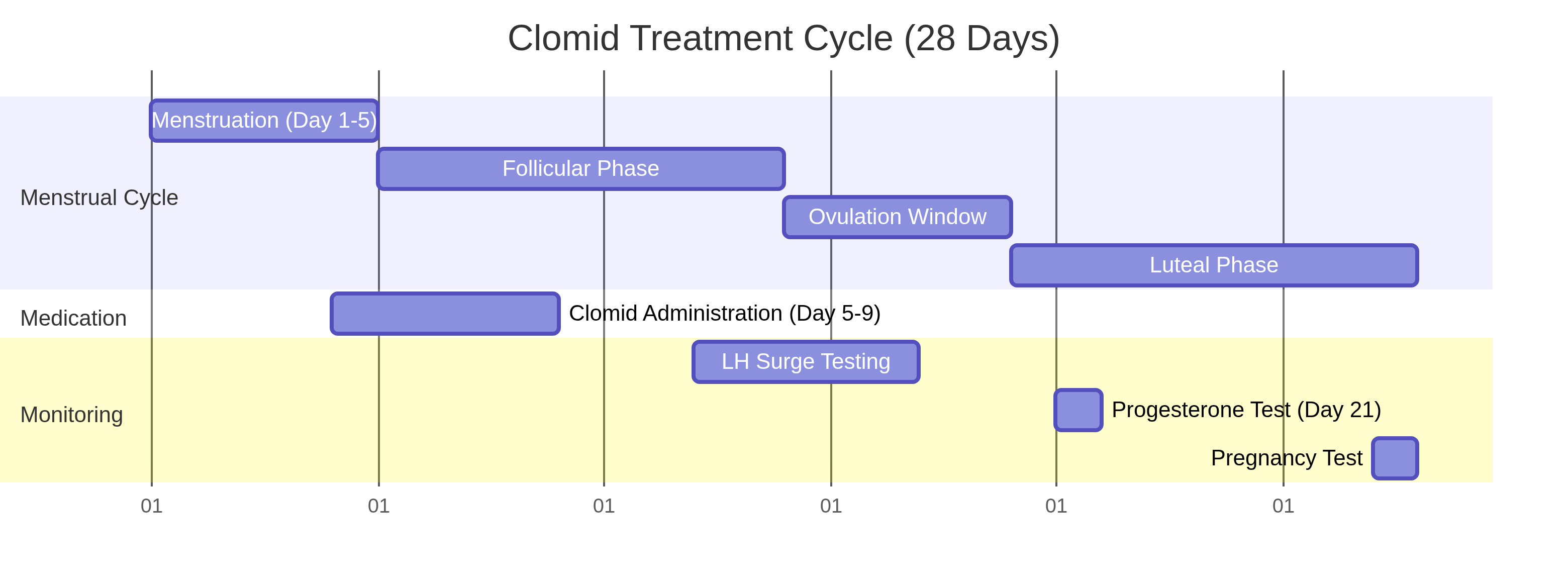
Transvaginal ultrasound is used to visualize the ovaries and measure the size and number of developing follicles. A baseline ultrasound is often performed on Day 2 or 3 of the menstrual cycle to ensure there are no pre-existing cysts. Follow-up ultrasounds are usually scheduled around Day 10 to 12 to track follicular growth. A mature follicle ready for ovulation typically measures between 18 and 24 millimeters in diameter. Ultrasound also allows the physician to assess the thickness and pattern of the endometrial lining, which must be adequately developed to support implantation.
Blood tests are used to measure hormone levels, providing a biochemical picture of the cycle. Estradiol levels rise as the follicles grow, giving an indication of their maturity and the overall ovarian response. A sudden surge in Luteinizing Hormone (LH) triggers ovulation, and this can be detected via blood tests or home urine ovulation predictor kits. About a week after suspected ovulation, a serum progesterone level is checked to confirm that ovulation has indeed occurred and that the corpus luteum is functioning properly.
25mg (Low Dose / Off-label)
A 25mg dose is considered a low or off-label starting dose. It is sometimes used for women who are particularly sensitive to fertility medications or those who have experienced severe side effects at higher doses. In some cases, it is also used off-label for male infertility to stimulate testosterone production without overstimulating the system. This dose requires careful monitoring to ensure it is effective without causing adverse reactions.
The rationale for using a 25mg dose in women is often to minimize the anti-estrogenic side effects of Clomid, particularly its negative impact on cervical mucus and the endometrial lining. By using the lowest effective dose, physicians aim to induce ovulation while maintaining a hospitable environment for sperm transport and embryo implantation. This approach is particularly relevant for women who have a robust ovarian reserve and are at a higher risk of over-responding to standard doses.
In the context of male infertility, the 25mg dose is frequently employed to gently stimulate the HPG axis. Men are often more sensitive to the effects of Clomid than women, and higher doses can lead to an excessive increase in estrogen levels, which can paradoxically suppress testosterone production and impair spermatogenesis. A low, carefully titrated dose helps maintain the delicate balance of androgens and estrogens necessary for optimal male reproductive function.
50mg (Standard Starting Dose)
The 50mg dose is the standard, FDA-approved starting dose for ovulation induction in women. A typical protocol involves taking 50mg daily for five consecutive days, usually beginning on Day 3, 4, or 5 of the menstrual cycle. This dose is effective for the majority of women with ovulatory dysfunction, particularly those with PCOS. If ovulation occurs but pregnancy is not achieved, the 50mg dose is usually maintained for subsequent cycles.
The choice of which day to start the medication (Day 3, 4, or 5) can vary depending on the physician's preference and the patient's specific diagnosis. Starting earlier in the cycle (Day 3) may recruit more follicles, potentially increasing the chances of a multiple pregnancy, while starting later (Day 5) may result in the development of a single, dominant follicle. Regardless of the start day, the five-day course is designed to provide a sufficient stimulus to the hypothalamus to initiate the cascade of events leading to ovulation.
If a patient ovulates on the 50mg dose but does not conceive, there is generally no benefit to increasing the dose in subsequent cycles. The goal of Clomid therapy is to achieve ovulation, and once that is accomplished, higher doses will not improve pregnancy rates and will only increase the risk of side effects. Instead, the physician may recommend continuing the 50mg dose for up to three to six cycles, or adding other interventions such as Intrauterine Insemination (IUI) to enhance the chances of success.
100mg (Adjusted Therapeutic Dose)
If a patient does not ovulate on the standard 50mg dose, the physician may increase the dosage to 100mg daily for five days in the next cycle. This adjusted therapeutic dose is designed to provide a stronger stimulus to the hypothalamus and pituitary gland. Doses higher than 100mg are rarely recommended, as they do not significantly improve ovulation rates but do increase the risk of side effects, including visual disturbances and OHSS.
The decision to increase the dose to 100mg is based on the patient's lack of response to the initial 50mg trial. This lack of response, known as Clomid resistance, is relatively common, particularly among women with PCOS who have high body mass indices (BMI) or severe insulin resistance. The higher dose aims to overcome this resistance by more aggressively blocking estrogen receptors and forcing a stronger GnRH pulse.
If a patient fails to ovulate on the 100mg dose, some physicians may cautiously try a 150mg dose, although this is less common and carries a higher risk profile. If ovulation is still not achieved, the patient is considered Clomid-resistant, and alternative treatments must be explored. These alternatives may include adding an insulin-sensitizing medication like metformin, switching to an aromatase inhibitor like letrozole, or moving to injectable gonadotropins.
Generic vs. Brand Name Clomid
When considering Clomid, patients often wonder about the differences between the brand-name medication and its generic counterpart, clomiphene citrate. Both versions contain the exact same active ingredient and are designed to work identically in the body to induce ovulation.
Brand Name (Clomid): Originally developed and patented, the brand-name version is often more expensive due to the costs associated with research, development, and marketing. Some patients and doctors prefer the brand name due to familiarity and long-standing trust in the specific manufacturer. The brand name Clomid was first approved by the FDA in 1967 and has a long history of clinical use and extensive safety data backing its efficacy.
Generic (Clomiphene Citrate): The generic version is chemically equivalent to the brand name and must meet the same strict FDA standards for safety, efficacy, and quality. Generic clomiphene citrate is typically much more affordable and is widely available. Many insurance plans prefer or require the use of the generic version to keep out-of-pocket costs low. The FDA requires that generic drugs have the same active ingredient, strength, dosage form, and route of administration as the brand-name product. They must also prove bioequivalence, meaning they are absorbed into the bloodstream at the same rate and to the same extent as the original drug.
While the active ingredient is identical, the inactive ingredients (excipients) such as binders, fillers, and dyes may differ between the brand name and generic versions. In rare cases, a patient may have an allergy or sensitivity to a specific inactive ingredient in one formulation but not the other. However, for the vast majority of patients, generic clomiphene citrate is just as safe and effective as brand-name Clomid.
Ultimately, the choice between generic and brand name should be discussed with your healthcare provider, taking into account your insurance coverage and personal preferences. Both are highly effective options for treating ovulatory dysfunction, and the cost savings associated with the generic version make it the preferred choice for many patients undergoing fertility treatment.
Purchasing Clomid: Cost, Legal Acquisition, and Counterfeit Prevention
The cost of Clomid without insurance typically ranges from $20 to $100 per cycle for the generic version (clomiphene citrate). Brand-name Clomid may be more expensive. The only legal and safe way to obtain Clomid is through a valid prescription from a licensed healthcare provider.
The financial aspect of fertility treatment can be a significant burden for many couples. Fortunately, Clomid is one of the most affordable fertility medications available, especially when compared to the high costs of injectable gonadotropins or In Vitro Fertilization (IVF). Many health insurance plans cover the cost of Clomid, particularly if it is prescribed to treat an underlying medical condition like PCOS rather than solely for infertility. Patients should check with their insurance provider to understand their specific coverage and copay requirements.
To avoid the significant risks of counterfeit pharmacies, only purchase from reputable, licensed pharmacies. Avoid online 'no-prescription' pharmacies, as their products are often unregulated, potentially contaminated, or contain incorrect dosages. Look for pharmacies verified by the National Association of Boards of Pharmacy (NABP) or those that require a consultation with a licensed pharmacist.
The dangers of purchasing prescription medications from unverified online sources cannot be overstated. Counterfeit drugs may contain no active ingredient, the wrong active ingredient, or dangerous impurities. In the case of Clomid, taking a counterfeit product could not only fail to induce ovulation but could also cause severe hormonal imbalances or toxic reactions. Always ensure that the pharmacy you use requires a valid prescription from your doctor and provides a way to contact a pharmacist with any questions or concerns.
Official Instructions and Guidelines
It is imperative to follow the official prescribing information and guidelines provided by your healthcare professional and the FDA. The standard protocol involves taking the medication at the same time each day for the prescribed five-day period. If you miss a dose, contact your doctor immediately for instructions; do not double the dose to catch up.
The timing of intercourse is a critical component of Clomid therapy. Because Clomid induces ovulation, it is essential that sperm are present in the reproductive tract when the egg is released. Your doctor will likely advise you to have intercourse every other day starting a few days before expected ovulation and continuing for a few days after. This ensures a steady supply of viable sperm ready to fertilize the egg.
During treatment, you may be advised to use ovulation predictor kits or undergo ultrasound monitoring to determine the optimal time for intercourse or intrauterine insemination (IUI). Ovulation predictor kits detect the surge in Luteinizing Hormone (LH) that precedes ovulation by 24 to 36 hours. This provides a clear window of peak fertility. Ultrasound monitoring offers a more precise assessment of follicular development and can help your doctor pinpoint the exact day of ovulation.
Always report any unusual symptoms, especially visual changes or severe abdominal pain, to your doctor promptly. These could be signs of serious complications such as visual disturbances or Ovarian Hyperstimulation Syndrome (OHSS). Do not ignore these symptoms or assume they are normal side effects of the medication. Early detection and management are crucial for preventing long-term consequences.
Alternatives: Letrozole, Gonadotropins, and IVF
If Clomid does not result in a successful pregnancy, several alternatives are available. Letrozole (Femara) is an aromatase inhibitor that is increasingly used as a first-line treatment for women with PCOS, as some studies suggest it may have higher live-birth rates and a lower risk of multiples in that specific population. Letrozole works by temporarily suppressing estrogen production, which stimulates the pituitary gland to release more FSH. Unlike Clomid, letrozole does not deplete estrogen receptors, so it typically does not have the same negative effects on cervical mucus and the endometrial lining.
Gonadotropins are injectable hormones that directly stimulate the ovaries; these are more powerful but carry a higher risk of OHSS and multiple births. Gonadotropins contain FSH, LH, or a combination of both, and are administered via subcutaneous injection. They are often used for women who are Clomid-resistant or those undergoing advanced fertility treatments like IVF. Because gonadotropins directly stimulate the ovaries, they require intense monitoring with frequent ultrasounds and blood tests to carefully titrate the dose and prevent overstimulation.
Finally, In Vitro Fertilization (IVF) is the most advanced option, where eggs are retrieved and fertilized in a lab before being transferred back to the uterus. IVF is typically recommended for couples with severe male factor infertility, blocked fallopian tubes, advanced maternal age, or unexplained infertility that has not responded to other treatments. While IVF is the most invasive and expensive option, it also offers the highest per-cycle success rates.
The choice of treatment depends on the underlying cause of infertility, the patient's age, and their response to previous therapies. A thorough discussion with a reproductive endocrinologist is essential to determine the most appropriate and effective treatment plan for each individual couple.
When to Call Your Doctor
Close communication with your fertility specialist is vital. You should call your doctor immediately if you experience any of the following: severe pelvic pain or pressure, sudden and rapid weight gain (more than 5 pounds in two days), shortness of breath, decreased urination, or any changes in your vision, such as blurring or seeing flashes. These could be signs of OHSS or other serious complications that require urgent medical evaluation.
It is also important to contact your doctor if you experience severe nausea, vomiting, or diarrhea, as these can lead to dehydration and exacerbate the symptoms of OHSS. If you develop a severe headache that does not respond to over-the-counter pain relievers, or if you experience any signs of an allergic reaction, such as rash, itching, swelling of the face or throat, or difficulty breathing, seek immediate medical attention.
Furthermore, if you suspect you may be pregnant while taking Clomid, stop the medication immediately and contact your doctor. Clomid is contraindicated during pregnancy and can cause harm to the developing fetus. A blood test can confirm pregnancy and allow your doctor to provide appropriate prenatal care.
Government and Regulatory Resources
For more detailed information, official guidelines, and regulatory updates regarding Clomid (clomiphene citrate), please refer to the following government and authoritative resources:
- FDA Prescribing Information for Clomid (PDF) - The official FDA label detailing indications, dosage, contraindications, and clinical pharmacology.
- NCBI StatPearls: Clomiphene Overview - A comprehensive clinical overview of clomiphene citrate provided by the National Center for Biotechnology Information.
- Mayo Clinic: Clomiphene (Oral Route) Information - Patient-friendly information on the uses, side effects, and precautions associated with clomiphene.
- WHO Model Lists of Essential Medicines - Information on clomiphene's inclusion in the World Health Organization's list of essential medicines.
Editorial Review & Medical Sources
This guide is for informational purposes and does not constitute medical advice. Content is based on clinical data from the FDA, the American Society for Reproductive Medicine (ASRM), and the Mayo Clinic. Medical Reviewer: Dr. Sanjai Sinha, MD. Primary Sources: FDA Prescribing Information, ASRM Patient Guides, Clinical Trials Database (NCBI).
Clomid Quick View
| Active Ingredient | Clomiphene Citrate |
|---|---|
| Manufacturer | Sanofi-Aventis / Various Generics |
| Type | Selective Estrogen Receptor Modulator (SERM) |
| Onset | Ovulation typically 5-10 days after last dose |
| Duration | One treatment cycle |
| Food Interaction | No restrictions; take with a full glass of water |
| Alcohol | Avoid; alcohol can exacerbate dizziness and mood swings |
| Prescription | Required (Strict Medical Supervision) |
Clomid Side Effects
Common Side Effects
- Vasomotor flushes (Hot flashes) - ~10% of users.
- Abdominal discomfort, bloating, or pelvic pressure.
- Breast tenderness or mastalgia.
- Nausea and mild gastrointestinal upset.
- Headache and dizziness.
- Mood swings and emotional sensitivity ('Clomid Crazies').
Uncommon Side Effects
- Visual disturbances (blurring, spots, or flashes of light).
- Ovarian enlargement (mild to moderate).
- Intermenstrual spotting.
- Reversible hair thinning.
- Insomnia and increased anxiety.
Rare Side Effects
- Ovarian Hyperstimulation Syndrome (OHSS) - Risk is <1%.
- Multiple gestations - Twins occur in 5-8% of cases.
- Ovarian torsion.
- Severe allergic reactions (Anaphylaxis).
Important Warning: CRITICAL SAFETY WARNING: If you experience any change in your vision, stop taking Clomid immediately. Seek emergency care for severe pelvic pain or rapid weight gain.
More Information About Clomid
Storage
Store at controlled room temperature (15°C to 30°C / 59°F to 86°F). Protect from heat, light, and excessive moisture.
Contraindications
Clomid is strictly contraindicated in: 1. Pregnancy (Category X). 2. Liver disease or history of hepatic dysfunction. 3. Undiagnosed abnormal uterine bleeding. 4. Ovarian cysts not related to PCOS. 5. Uncontrolled thyroid or adrenal dysfunction. 6. Known hypersensitivity to clomiphene.
Drug Interactions
While Clomid has few direct drug-drug interactions, it should not be combined with other ovulation-inducing agents (like Letrozole or Gonadotropins) unless under strict specialist supervision. Inform your doctor of all supplements, especially herbal products like Vitex (Chasteberry), which can interfere with the hormonal feedback loop.
Clomid FAQs
About 80% of women with PCOS will ovulate on Clomid. Cumulative pregnancy rates are around 45% after 6 cycles.
Yes, it is a common side effect caused by anti-estrogenic effects on the brain. It is temporary.
Yes, it is used off-label to boost natural testosterone and improve sperm parameters, but must be monitored by a doctor.
No, Clomid is a prescription-only medication. Buying it without a prescription is illegal and dangerous.
Written and Reviewed by Our Qualified Team

Find out more about our medical content authors and how we ensure the accuracy of our content.
Content last updated: 19 May 2026
Clomid Reviews
Based on 37 reviews
I've tried other options, but Clomid is by far the best. Great quality and results.
Clomid is a fantastic product. It's helped me immensely and I'd recommend it to anyone.
Initially skeptical, but Clomid proved me wrong. It's effective and I'm happy with it.
Very satisfied with my experience using Clomid. It's reliable and consistent.
Very satisfied with my experience using Clomid. It's reliable and consistent.
Clomid is a fantastic product. It's helped me immensely and I'd recommend it to anyone.
Clomid is a fantastic product. It's helped me immensely and I'd recommend it to anyone.
Clomid has been a game-changer. I feel so much better since starting it.
Highly recommend Clomid! It worked wonders for me. So glad I found it.
Highly recommend Clomid! It worked wonders for me. So glad I found it.
Initially skeptical, but Clomid proved me wrong. It's effective and I'm happy with it.
Couldn't be happier with Clomid. It's easy to use and the benefits are clear.
Clomid has been a game-changer. I feel so much better since starting it.
Couldn't be happier with Clomid. It's easy to use and the benefits are clear.
Couldn't be happier with Clomid. It's easy to use and the benefits are clear.
Very satisfied with my experience using Clomid. It's reliable and consistent.
I've tried other options, but Clomid is by far the best. Great quality and results.
I've tried other options, but Clomid is by far the best. Great quality and results.
Clomid has been a game-changer. I feel so much better since starting it.
Initially skeptical, but Clomid proved me wrong. It's effective and I'm happy with it.
Highly recommend Clomid! It worked wonders for me. So glad I found it.
Initially skeptical, but Clomid proved me wrong. It's effective and I'm happy with it.
Clomid is a fantastic product. It's helped me immensely and I'd recommend it to anyone.
Highly recommend Clomid! It worked wonders for me. So glad I found it.
If you're considering Clomid, go for it! You won't be disappointed. It's truly effective.
Initially skeptical, but Clomid proved me wrong. It's effective and I'm happy with it.
If you're considering Clomid, go for it! You won't be disappointed. It's truly effective.
A solid 5 stars for Clomid. It exceeded my expectations and delivered on its promises.
Clomid helped me conceive after 2 years of trying. Started ovulating regularly within the first cycle.
Clomid helped me conceive after 2 years of trying. Started ovulating regularly within the first cycle.
Clomid helped me conceive after 2 years of trying. Started ovulating regularly within the first cycle.
Clomid helped me conceive after 2 years of trying. Started ovulating regularly within the first cycle.
Experienced some mood swings and hot flashes but it was worth it. Pregnant after 3 cycles.
My fertility specialist prescribed Clomid and it worked wonderfully. Now 12 weeks pregnant!
Good medication for ovulation induction. Side effects were manageable. Currently on my second cycle.
After being diagnosed with PCOS, Clomid was the solution. Conceived naturally after 4 cycles.
Had significant side effects including bloating and headaches. Effective but not easy to tolerate.
Leave a Review
How Does It Work?
Research
Read our comprehensive review to understand the medication
Consult Your Doctor
Discuss the medication with your healthcare provider
Get Your Prescription
Obtain a valid prescription from your doctor