Neurontin (Pfizer)
General Health Treatment
Neurontin (Gabapentin) is a widely prescribed medication used to treat neuropathic pain, postherpetic neuralgia, and partial-onset seizures by modulating calcium channels in the central nervous system.
Table of Contents
Neurontin Product Information
What is Neurontin (Gabapentin)?
Neurontin, known generically as gabapentin, is a widely prescribed medication that belongs to a class of drugs called gabapentinoids. Originally developed and approved by the FDA in 1993 as an anticonvulsant to treat epilepsy, its clinical applications have expanded dramatically over the past three decades. Today, it is most frequently prescribed for the management of neuropathic pain—pain caused by damage or dysfunction in the nervous system.
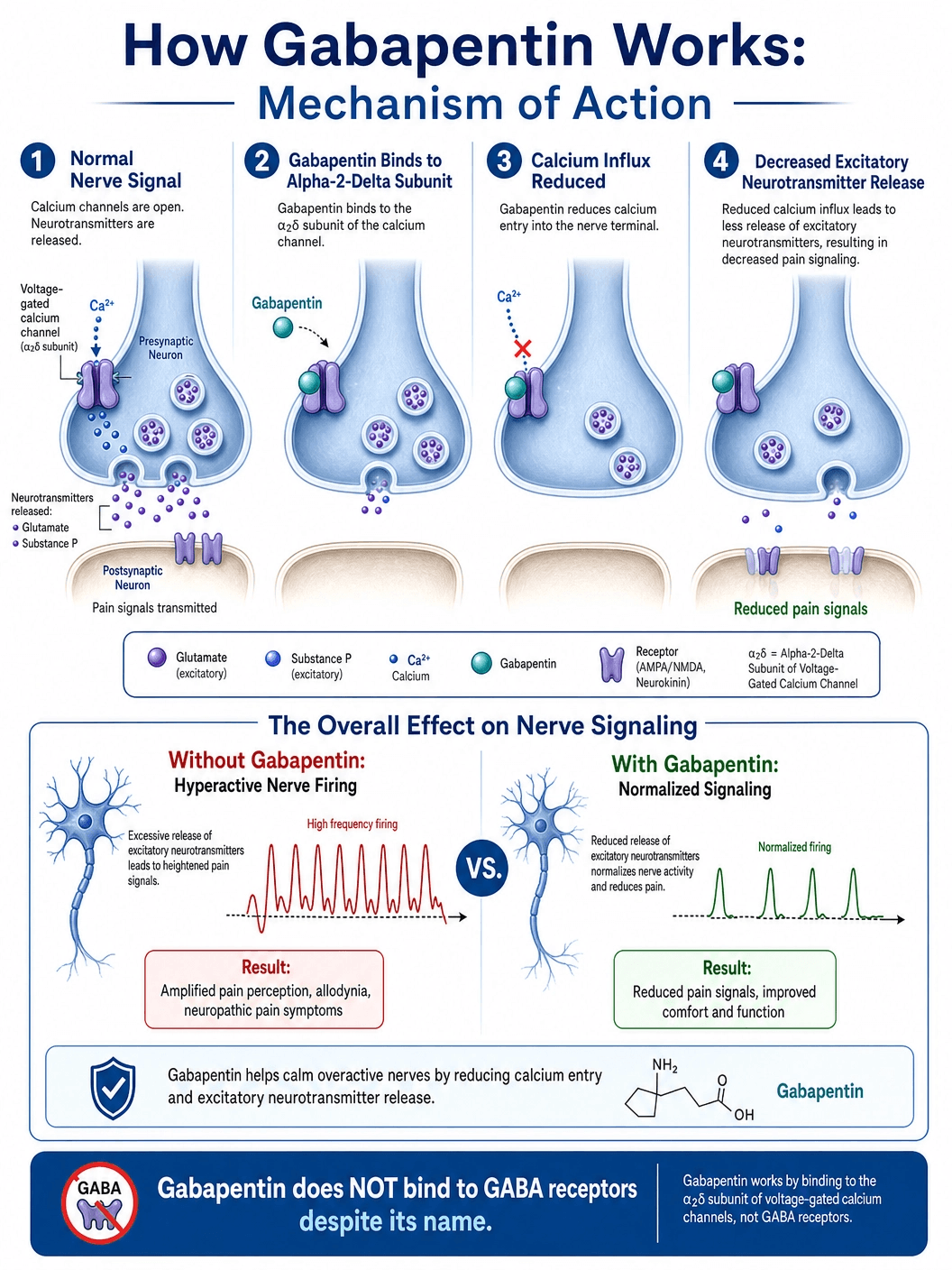
Despite its name, which suggests a relationship to the inhibitory neurotransmitter gamma-aminobutyric acid (GABA), gabapentin does not actually bind to GABA receptors, nor does it influence the synthesis or uptake of GABA. Instead, it works through a unique and highly specific mechanism involving calcium channels in the central nervous system, effectively "calming" overactive nerves that are misfiring and sending inappropriate pain or seizure signals to the brain.
Mechanism of Action: How Gabapentin Works
The precise mechanism by which gabapentin exerts its analgesic and anticonvulsant effects was a mystery for many years after its introduction. Modern pharmacology has since elucidated its primary target: the alpha-2-delta (α2δ) subunit of voltage-gated calcium channels.
The Role of Calcium Channels: In a healthy nervous system, when an electrical signal (action potential) reaches the end of a nerve cell, voltage-gated calcium channels open. The influx of calcium ions triggers the release of excitatory neurotransmitters, such as glutamate, substance P, and calcitonin gene-related peptide (CGRP), which carry the signal across the synapse to the next nerve cell. In conditions like epilepsy or neuropathic pain, these nerves become hyperexcitable, firing too frequently and releasing excessive amounts of these excitatory chemicals.
The Gabapentin Blockade: Gabapentin binds with high affinity to the α2δ-1 and α2δ-2 subunits of these calcium channels in the brain and spinal cord. By binding to this specific site, gabapentin reduces the influx of calcium into the nerve terminal. This, in turn, significantly decreases the release of the excitatory neurotransmitters. Essentially, gabapentin acts as a dimmer switch for the nervous system, turning down the volume on hyperactive nerve signals without completely blocking normal nerve function.
FDA-Approved Indications
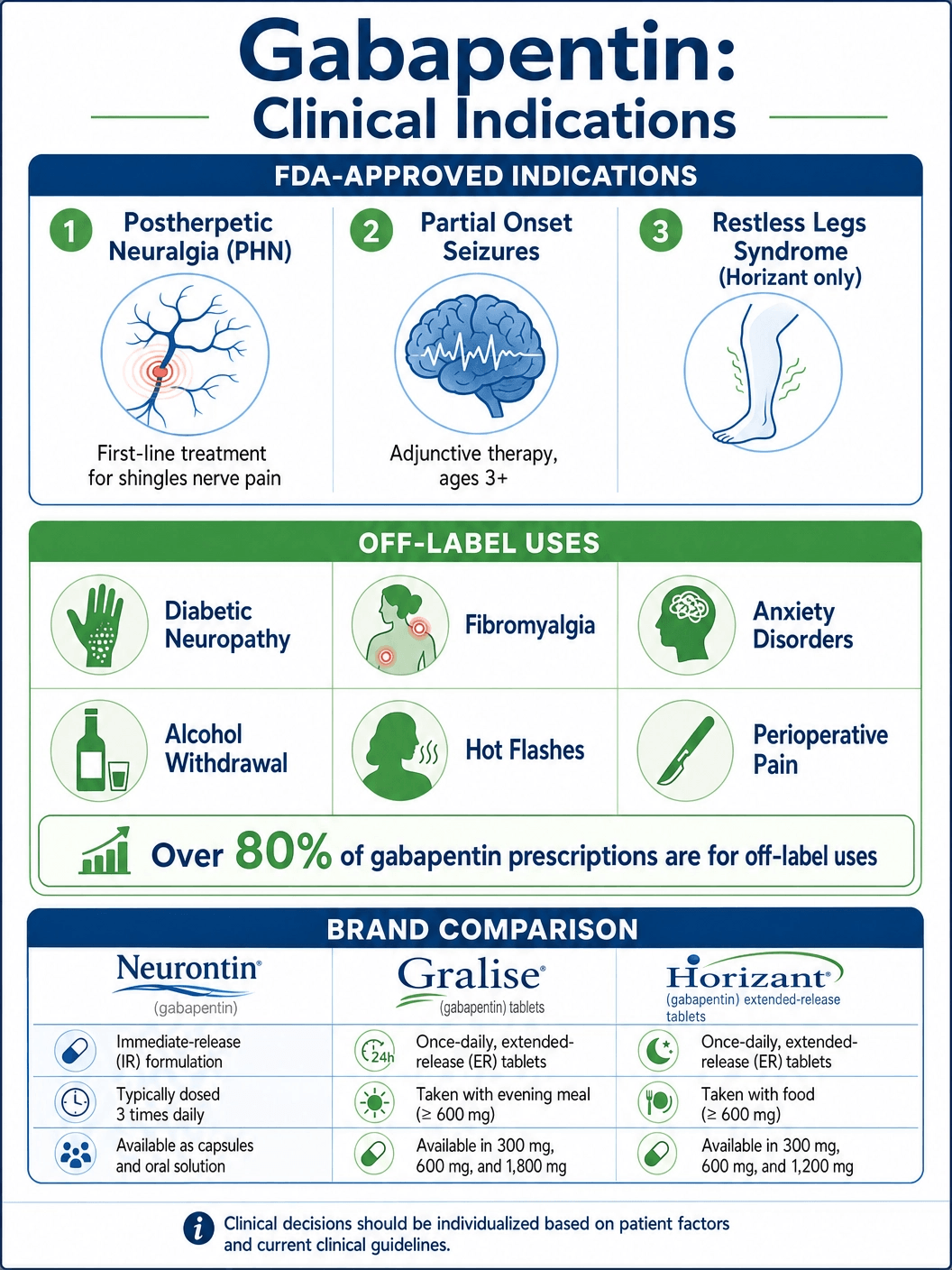
While gabapentin is used for a vast array of conditions, it currently holds FDA approval for only a specific set of neurological disorders.
Postherpetic Neuralgia (PHN): This is the most common FDA-approved use for gabapentin. PHN is a severe, chronic, burning, or stabbing nerve pain that persists for months or even years after an outbreak of shingles (Herpes zoster) has healed. The shingles virus damages the peripheral nerves, causing them to misfire continuously. Gabapentin is considered a first-line treatment for quieting these damaged nerves and providing significant pain relief.
Partial Onset Seizures: Gabapentin is approved as an adjunctive (add-on) therapy for the treatment of partial-onset seizures, with or without secondary generalization, in adults and pediatric patients 3 years of age and older. It is rarely used as a standalone (monotherapy) treatment for epilepsy, but it is highly effective when combined with other antiepileptic drugs.
Restless Legs Syndrome (RLS): A specific extended-release formulation of gabapentin enacarbil (brand name Horizant) is FDA-approved for the treatment of moderate-to-severe primary Restless Legs Syndrome. RLS is a neurological sleep disorder characterized by an irresistible urge to move the legs, usually accompanied by uncomfortable sensations, which severely disrupts sleep.
The Vast Landscape of Off-Label Use
Gabapentin is one of the most widely prescribed "off-label" medications in the world. Off-label use means a doctor prescribes the drug for a condition not explicitly approved by the FDA, based on clinical experience and emerging research. It is estimated that over 80% of gabapentin prescriptions are for off-label uses.
Diabetic Peripheral Neuropathy (DPN): While pregabalin (Lyrica) is FDA-approved for DPN, gabapentin is frequently used off-label as a first-line, lower-cost alternative to treat the burning, tingling nerve pain in the feet and legs caused by chronic high blood sugar.
Fibromyalgia: Similar to DPN, gabapentin is widely used to manage the widespread musculoskeletal pain, fatigue, and sleep disturbances associated with fibromyalgia.
Anxiety Disorders: Psychiatrists frequently prescribe gabapentin off-label for generalized anxiety disorder (GAD) and social anxiety disorder. Its calming effect on the central nervous system can help reduce racing thoughts and physical symptoms of anxiety without the addiction risks associated with benzodiazepines (like Xanax or Valium).
Alcohol Withdrawal and Dependence: Gabapentin is increasingly used in addiction medicine to manage the symptoms of mild to moderate alcohol withdrawal (such as tremors, anxiety, and insomnia) and to help reduce cravings and maintain abstinence in patients recovering from alcohol use disorder.
Other Pain Syndromes: It is also used for sciatica, trigeminal neuralgia, complex regional pain syndrome (CRPS), and to reduce the need for opioids in postoperative pain management.
Understanding the Side Effect Profile
Gabapentin is generally well-tolerated, especially when the dose is started low and increased gradually. However, because it acts on the central nervous system, it does have a distinct side effect profile.
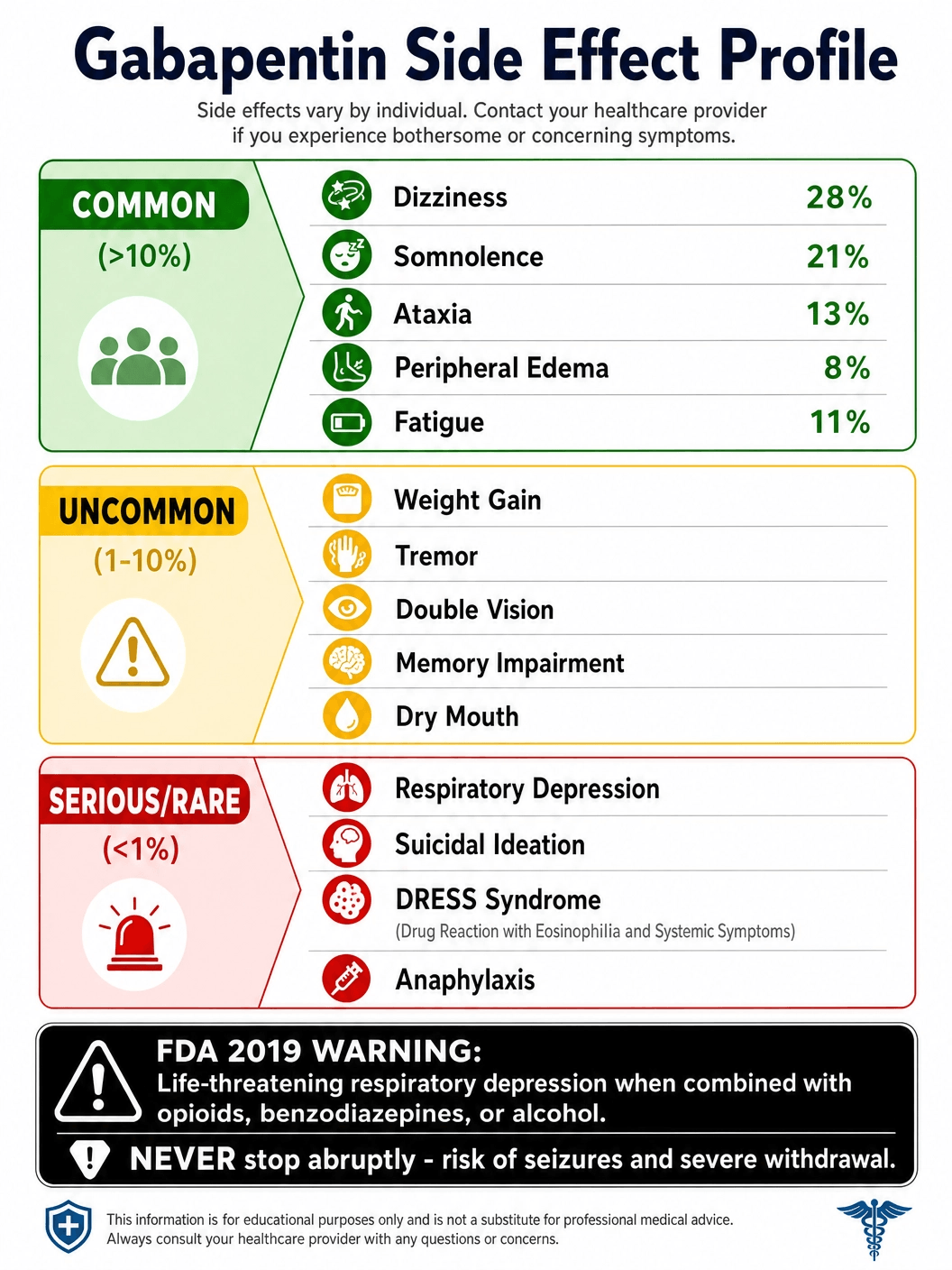
Common Side Effects: The most frequently reported side effects are dose-dependent and often subside as the body adjusts to the medication over a few weeks. These include:
- Dizziness and Ataxia: A feeling of unsteadiness, loss of coordination, or clumsiness.
- Somnolence (Drowsiness): Significant fatigue or sleepiness, which is why the largest dose is often taken at bedtime.
- Peripheral Edema: Swelling in the hands, legs, and feet due to fluid retention.
- Cognitive Effects: Some patients report "brain fog," difficulty concentrating, or mild memory impairment.
Serious but Rare Side Effects:
- Respiratory Depression: In 2019, the FDA issued a serious warning that gabapentinoids can cause life-threatening breathing difficulties, particularly in elderly patients, those with underlying lung conditions (like COPD), or when combined with other central nervous system depressants like opioids, benzodiazepines, or alcohol.
- Suicidal Ideation: Like all antiepileptic drugs, gabapentin carries a warning for a slightly increased risk of suicidal thoughts or behaviors. Patients and caregivers must monitor for sudden changes in mood, worsening depression, or unusual behavior.
- Severe Allergic Reactions: Though rare, gabapentin can cause DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms), a potentially fatal multi-organ hypersensitivity reaction characterized by fever, rash, and swollen lymph nodes.
The Importance of Tapering: Withdrawal Syndrome
Gabapentin must never be stopped abruptly. Even though it is not classified as a narcotic, the brain and nervous system adapt to its presence. Sudden discontinuation can trigger a severe withdrawal syndrome.
Withdrawal Symptoms: If stopped suddenly, patients may experience severe anxiety, insomnia, nausea, sweating, rapid heart rate, and a rebound of the pain or seizures the medication was treating. In patients taking gabapentin for epilepsy, abrupt cessation can trigger status epilepticus, a life-threatening state of continuous seizures.
The Tapering Protocol: To safely discontinue gabapentin, the dose must be gradually reduced over a minimum of one week, though many doctors prefer a slower taper over several weeks or months, depending on how long the patient has been taking the drug and at what dosage. This slow reduction allows the calcium channels and neurotransmitter levels to slowly return to their baseline state.
Available Dosages and Administration Guidelines
Gabapentin dosing is highly individualized. Because the drug's absorption in the gut is not linear (meaning taking a higher dose doesn't necessarily mean proportionally more drug enters the bloodstream), dosing must be carefully titrated.
Postherpetic Neuralgia (PHN) Dosing
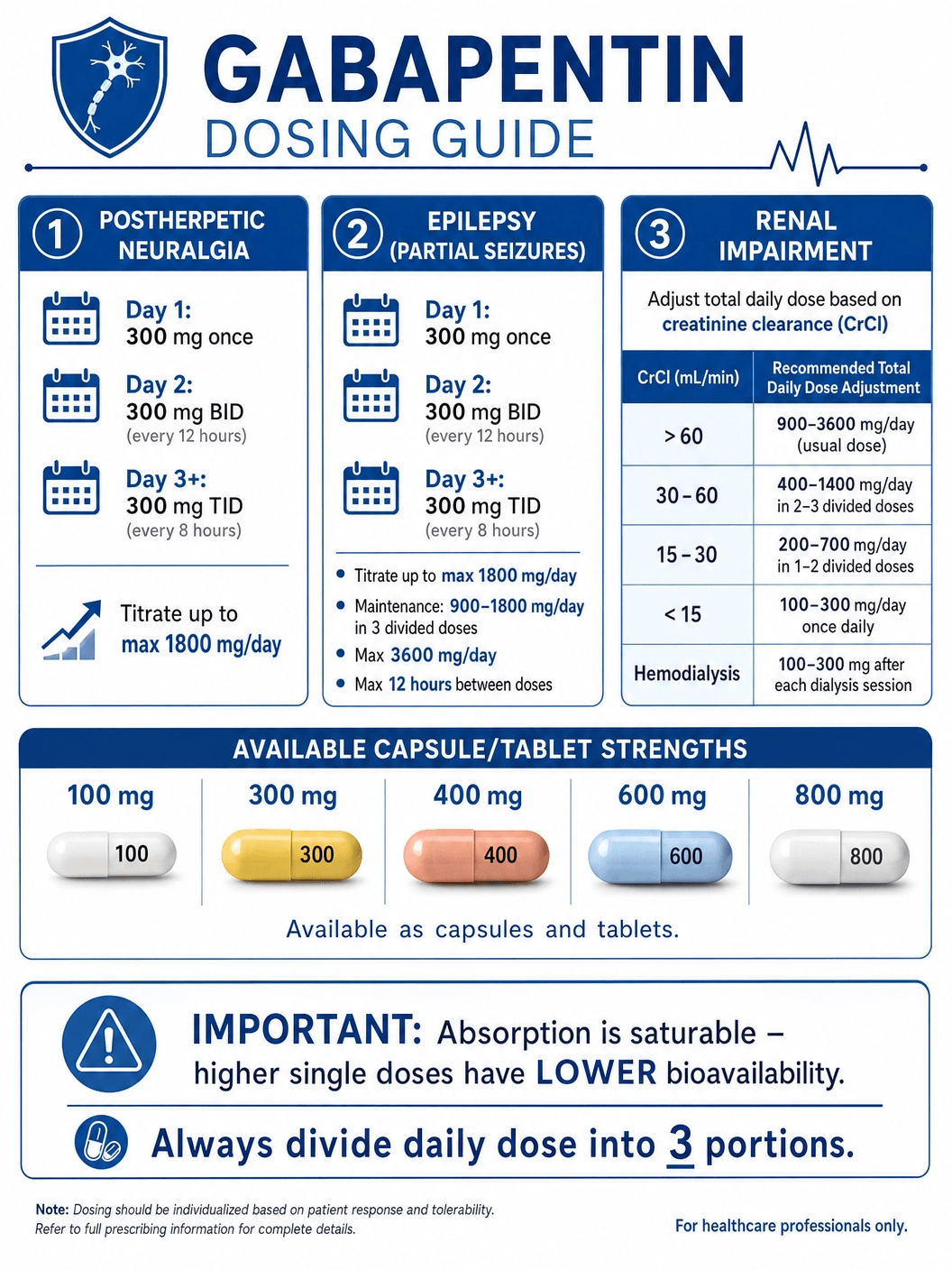
For nerve pain from shingles, the typical starting dose is 300 mg on Day 1, 300 mg twice a day on Day 2, and 300 mg three times a day on Day 3. The dose can then be titrated up as needed for pain relief, up to a maximum recommended dose of 1800 mg per day (divided into three 600 mg doses). Some patients may require higher doses, but absorption decreases significantly at higher amounts.
Epilepsy (Partial Seizures) Dosing
For adults and children over 12, the starting schedule is similar to PHN (reaching 300 mg three times a day by Day 3). The effective maintenance dose is usually between 900 mg and 1800 mg per day, divided into three doses. The maximum time between doses should not exceed 12 hours to prevent breakthrough seizures.
Renal Impairment Adjustments
Gabapentin is not metabolized by the liver; it is excreted entirely unchanged by the kidneys. Therefore, patients with impaired kidney function (reduced creatinine clearance) or those on hemodialysis must have their doses significantly reduced to prevent the drug from accumulating to toxic levels in the blood.
Generic vs. Brand Name Neurontin
The original patent for Neurontin, held by Pfizer, expired in 2004. Since then, generic gabapentin has become widely available and is the standard of care due to its low cost.
Generic Gabapentin: The FDA requires generic gabapentin to be bioequivalent to Neurontin, meaning it delivers the same amount of active ingredient into the bloodstream over the same period. For the vast majority of patients, generic gabapentin is just as safe and effective as the brand name.
Extended-Release Formulations: It is critical to note that standard gabapentin (Neurontin or generic) is not interchangeable with extended-release formulations like Gralise or Horizant.
- Gralise: An extended-release tablet approved only for postherpetic neuralgia. It is taken once daily with the evening meal.
- Horizant (gabapentin enacarbil): A prodrug of gabapentin designed to overcome the absorption limitations of standard gabapentin. It is approved for RLS and PHN.
Purchasing Neurontin: Cost, Insurance, and Legal Acquisition
Gabapentin is a prescription-only medication. While it is not federally scheduled as a controlled substance under the DEA in the United States, several individual states (such as Kentucky, Virginia, and Michigan) have reclassified it as a Schedule V controlled substance due to increasing reports of misuse and diversion, particularly in combination with opioids.
Cost and Insurance: Generic gabapentin is highly affordable. A one-month supply of standard doses often costs less than $15 to $20 out-of-pocket. It is covered as a Tier 1 generic by almost all Medicare, Medicaid, and commercial insurance plans. Brand-name Neurontin, Gralise, or Horizant are significantly more expensive and typically require prior authorization from insurance companies proving that the generic failed.
Legal Acquisition: Patients must obtain a valid prescription from a licensed healthcare provider. Due to state-level monitoring programs (PDMPs), pharmacists closely track gabapentin prescriptions to prevent doctor-shopping and dangerous drug combinations.
Gabapentin Misuse and the Opioid Epidemic
In recent years, gabapentin has come under intense scrutiny due to its role in the opioid epidemic. While gabapentin alone has a relatively low potential for abuse and addiction, it is frequently misused by individuals suffering from opioid use disorder.
The Synergistic High: When taken in massive doses alongside opioids (like heroin, fentanyl, or oxycodone), gabapentin significantly enhances the euphoric effects (the "high") of the opioid. It is also used by individuals to self-medicate through opioid withdrawal when they cannot obtain their drug of choice.
The Lethal Combination: This combination is incredibly dangerous. Both opioids and gabapentin depress the central nervous system. Taking them together exponentially increases the risk of severe respiratory depression, coma, and fatal overdose. This dangerous synergy is the primary reason many states have moved to track gabapentin prescriptions alongside traditional controlled substances.
Gabapentin vs. Pregabalin (Lyrica): Understanding the Difference
Gabapentin and pregabalin (Lyrica) are both gabapentinoids, working on the exact same α2δ calcium channel subunit. However, they have distinct pharmacokinetic differences that influence how they are prescribed.
Absorption and Bioavailability: The main difference lies in how the body absorbs them. Gabapentin's absorption is saturable; the transport proteins in the gut get "full," so taking a 1200mg dose does not result in twice as much drug in the blood as a 600mg dose. Pregabalin, on the other hand, has linear absorption. Its bioavailability is over 90% regardless of the dose, making it more predictable and allowing for twice-daily rather than three-times-daily dosing.
Potency and Scheduling: Pregabalin binds to the calcium channels with greater affinity, making it roughly 2.5 to 3 times more potent than gabapentin. Because of its rapid absorption and predictable high, pregabalin is federally classified as a Schedule V controlled substance across the entire United States, whereas gabapentin is only scheduled in certain states.
Government and Regulatory Resources
For the most accurate, up-to-date, and comprehensive information regarding gabapentin, patients and healthcare professionals should consult official government and regulatory resources:
- U.S. Food and Drug Administration (FDA): The FDA provides access to the official prescribing information, safety alerts (including the 2019 respiratory depression warning), and guidelines for all approved formulations of gabapentin. (fda.gov)
- National Institutes of Health (NIH) / DailyMed: DailyMed, provided by the National Library of Medicine, offers the most recent, comprehensive package inserts and labeling information submitted to the FDA. (dailymed.nlm.nih.gov)
- National Center for Biotechnology Information (NCBI): The NCBI's StatPearls database provides peer-reviewed, clinical overviews of gabapentin's pharmacology, indications, and adverse effects. (ncbi.nlm.nih.gov)
Gabapentin in Veterinary Medicine
Just as in human medicine, gabapentin has become an indispensable tool in veterinary practice, particularly for dogs and cats. Its safety profile and efficacy make it a go-to medication for several common veterinary issues.
Chronic Pain Management: Veterinarians frequently prescribe gabapentin to manage chronic neuropathic pain in pets, such as pain associated with osteoarthritis, intervertebral disc disease (IVDD), or cancer. It is often used as part of a multimodal pain management strategy, combined with NSAIDs (like carprofen or meloxicam) to provide comprehensive relief while minimizing the dose of any single drug.
Anxiety and Stress Reduction: One of the most common off-label uses of gabapentin in veterinary medicine is for acute anxiety, particularly in cats. A single dose given a few hours before a stressful event—such as a veterinary visit, a thunderstorm, or fireworks—can significantly reduce fear and aggression, making the experience safer and less traumatic for both the animal and the handler.
Seizure Control: While less commonly used as a primary anticonvulsant in pets compared to phenobarbital or levetiracetam, gabapentin is sometimes used as an add-on therapy for dogs or cats with refractory epilepsy that is not fully controlled by standard medications.
The Xylitol Warning: It is absolutely critical for pet owners to ensure that the liquid formulation of gabapentin they use does not contain xylitol. Xylitol is an artificial sweetener commonly used in human liquid medications to improve taste, but it is highly toxic to dogs, causing a rapid, life-threatening drop in blood sugar and severe liver damage. Veterinary-specific compounded liquids must always be used.
The Pharmacokinetics of Gabapentin: The Absorption Bottleneck
Understanding how the body processes gabapentin is crucial for understanding why it is dosed the way it is. The pharmacokinetics of gabapentin are unique and somewhat counterintuitive.
Saturable Absorption: Gabapentin is absorbed from the gastrointestinal tract into the bloodstream via a specific amino acid transporter (the L-amino acid transporter). The critical issue is that there are a limited number of these transporters in the gut. As the dose of gabapentin increases, these transporters become saturated (full). Therefore, the bioavailability (the percentage of the drug that actually reaches the blood) decreases as the dose increases. For example, a 300 mg dose might have a bioavailability of 60%, but an 800 mg dose might only have a bioavailability of 34%. This is why taking a massive dose of gabapentin all at once is inefficient and why the daily dose must be divided into three smaller doses throughout the day.
Lack of Hepatic Metabolism: Unlike many drugs that are broken down by the liver, gabapentin is not metabolized in humans. It does not induce or inhibit liver enzymes (like the Cytochrome P450 system). This is a significant clinical advantage because it means gabapentin has very few pharmacokinetic drug-drug interactions. It will not alter the blood levels of other medications the patient is taking.
Renal Excretion: Because it is not metabolized, gabapentin is eliminated from the body entirely unchanged through the kidneys into the urine. Its elimination half-life is relatively short, about 5 to 7 hours in patients with normal kidney function. This short half-life necessitates the three-times-daily dosing schedule to maintain stable blood levels and prevent breakthrough pain or seizures.
Gabapentin and Pregnancy: Weighing the Risks
The use of gabapentin during pregnancy presents a complex clinical dilemma, requiring a careful risk-benefit analysis by the patient and her healthcare provider.
Fetal Risks and Registry Data: Gabapentin crosses the human placenta. Animal studies have shown evidence of fetal toxicity (such as delayed bone ossification and increased fetal loss) at doses similar to human therapeutic doses. However, data from human pregnancy registries (such as the North American Antiepileptic Drug Pregnancy Registry) have not shown a definitive, significant increase in the risk of major congenital malformations compared to the general population. It is generally considered safer than older antiepileptic drugs like valproic acid, but it is not entirely without risk.
Neonatal Withdrawal: If a mother takes gabapentin late in pregnancy, the newborn may experience neonatal withdrawal syndrome after birth. Symptoms in the infant can include irritability, excessive crying, tremors, and feeding difficulties. These infants require close monitoring in a neonatal intensive care unit (NICU).
The Clinical Decision: The decision to use gabapentin during pregnancy depends heavily on the condition being treated. If the mother is taking it for epilepsy, uncontrolled seizures pose a massive risk of trauma and hypoxia to both the mother and the fetus, usually outweighing the risks of the medication. If it is being used for neuropathic pain, the provider may attempt to taper the drug or switch to safer alternatives, if possible.
Managing the Cognitive and Emotional Impact
While the physical side effects like dizziness are well-known, the cognitive and emotional impacts of gabapentin can be equally challenging for patients, particularly those on high doses or long-term therapy.
The "Brain Fog" Phenomenon: Many patients report a pervasive sense of cognitive dulling, often described as "brain fog." This can manifest as difficulty finding the right words (aphasia), short-term memory lapses, decreased attention span, and a general feeling of mental sluggishness. This can significantly impact a patient's ability to work, study, or manage complex daily tasks.
Emotional Blunting vs. Mood Swings: The drug's dampening effect on the nervous system can sometimes lead to emotional blunting—a feeling of apathy or being disconnected from one's emotions. Conversely, some patients experience the opposite: increased irritability, mood swings, or symptoms of depression. As mentioned earlier, the FDA requires a warning regarding the increased risk of suicidal ideation, making close psychiatric monitoring essential.
Mitigation Strategies: If cognitive or emotional side effects become intolerable, patients should never stop the medication abruptly. Instead, they should consult their physician. Strategies may include a slow dose reduction, shifting the largest dose to bedtime so the peak cognitive effects occur during sleep, or exploring alternative medications (like SNRIs for nerve pain) that may have a different side effect profile.
Gabapentin in the Context of Perioperative Care
In recent years, gabapentin has found a significant role in the surgical setting, specifically within Enhanced Recovery After Surgery (ERAS) protocols. These protocols aim to optimize patient outcomes, reduce hospital stays, and minimize the use of postoperative opioids.
Preemptive Analgesia: The concept of preemptive analgesia involves administering pain medication before the surgical incision is made, with the goal of preventing the central nervous system from becoming sensitized to the pain signals generated by the surgery. Gabapentin is frequently given as a single oral dose (e.g., 300 mg to 600 mg) 1 to 2 hours before surgery. By blocking the α2δ calcium channels preemptively, it reduces the hyperexcitability of the spinal cord that normally occurs in response to surgical trauma.
Opioid-Sparing Effects: Numerous clinical trials have demonstrated that administering gabapentin perioperatively significantly reduces the amount of opioid medication (like morphine or fentanyl) a patient requires in the first 24 to 48 hours after surgery. This opioid-sparing effect is crucial because it reduces the incidence of opioid-related side effects, such as severe nausea, vomiting, constipation, and respiratory depression, thereby accelerating the patient's recovery and discharge.
Postoperative Nausea and Vomiting (PONV): Interestingly, in addition to reducing pain, preoperative gabapentin has been shown to decrease the incidence of postoperative nausea and vomiting. While the exact mechanism for this antiemetic effect is not fully understood, it is likely related to its ability to reduce opioid consumption and its general dampening effect on the central nervous system.
The Role of Gabapentin in Psychiatry
While not FDA-approved for any psychiatric condition, gabapentin has become a heavily utilized tool in the psychiatric pharmacopeia, often serving as a safer alternative to traditional sedatives.
Anxiety Disorders: For patients with Generalized Anxiety Disorder (GAD) or Social Anxiety Disorder who do not respond to or cannot tolerate SSRIs (like Lexapro or Zoloft), gabapentin offers a viable alternative. Unlike benzodiazepines (like Xanax or Klonopin), which carry a high risk of tolerance, dependence, and severe withdrawal, gabapentin has a much lower abuse potential. It provides a generalized calming effect, reducing the physical symptoms of anxiety (racing heart, tension) and allowing patients to engage more effectively in cognitive behavioral therapy (CBT).
Bipolar Disorder: In the past, gabapentin was investigated as a potential mood stabilizer for bipolar disorder. However, large-scale clinical trials failed to show significant efficacy in treating acute mania or preventing manic episodes. Today, it is rarely used as a primary mood stabilizer, but it may be used adjunctively to manage comorbid anxiety or insomnia in bipolar patients.
Insomnia: Because somnolence is a primary side effect, gabapentin is frequently prescribed off-label for insomnia, particularly when the sleep disturbance is driven by chronic pain, restless legs syndrome, or severe anxiety. It has been shown to increase slow-wave (deep) sleep, improving overall sleep quality without the severe hangover effect often associated with traditional "Z-drugs" (like Ambien).
Gabapentin and the Elderly: A Cautionary Approach
Prescribing gabapentin to geriatric patients requires extreme caution and significant dose adjustments due to age-related physiological changes.
Decreased Renal Function: As humans age, kidney function naturally declines, even in the absence of overt kidney disease. Because gabapentin is cleared entirely by the kidneys, an elderly patient will clear the drug much more slowly than a younger adult. If an elderly patient is given a standard adult dose, the drug will accumulate in their bloodstream, leading to severe toxicity.
Increased Sensitivity to CNS Effects: The aging brain is more sensitive to medications that depress the central nervous system. Elderly patients are at a much higher risk of experiencing severe dizziness, ataxia (loss of coordination), and profound sedation when taking gabapentin. This significantly increases their risk of falls, which can lead to devastating consequences such as hip fractures or traumatic brain injuries.
The "Start Low, Go Slow" Paradigm: When treating elderly patients for conditions like postherpetic neuralgia, physicians must adhere strictly to the "start low and go slow" principle. The starting dose may be as low as 100 mg once daily, with very gradual upward titration based on the patient's clinical response and tolerability. Regular monitoring of renal function (via serum creatinine and estimated glomerular filtration rate) is mandatory.
The Future of Gabapentinoids
The widespread use and subsequent scrutiny of gabapentin have spurred ongoing research into the α2δ calcium channel subunit and the development of next-generation gabapentinoids.
Mirogabalin: Approved in Japan (but not currently in the US or Europe), mirogabalin is a newer gabapentinoid designed to bind more selectively and potently to the α2δ-1 and α2δ-2 subunits. The goal is to provide superior pain relief for conditions like diabetic peripheral neuropathy and postherpetic neuralgia while minimizing the central nervous system side effects (like dizziness and somnolence) that limit the use of gabapentin and pregabalin.
Targeted Delivery Systems: Researchers are also exploring novel delivery systems for gabapentin, such as topical creams or patches for localized neuropathic pain. By applying the medication directly to the affected area, high local concentrations could be achieved while minimizing systemic absorption, thereby avoiding the cognitive and sedative side effects entirely.
Redefining the Role in Pain Management: As the medical community continues to grapple with the opioid epidemic, the role of gabapentinoids is being constantly re-evaluated. While they remain crucial tools for neuropathic pain, the growing awareness of their misuse potential and respiratory risks (especially when combined with opioids) is leading to more stringent prescribing guidelines and a push for truly multimodal, non-pharmacological pain management strategies.
Gabapentin and the Management of Hot Flashes
One of the more surprising and highly effective off-label uses for gabapentin is in the management of vasomotor symptoms, commonly known as hot flashes, particularly in women who cannot or choose not to use hormone replacement therapy (HRT).
The Menopausal Transition: During menopause, the decline in estrogen levels disrupts the body's thermoregulatory center in the hypothalamus. This disruption causes the brain to incorrectly perceive that the body is overheating, triggering a sudden, intense flush of heat, sweating, and rapid heartbeat. For many women, these hot flashes are severe enough to disrupt sleep and significantly impair quality of life.
Breast Cancer Survivors: Gabapentin is especially critical for breast cancer survivors. Many breast cancers are hormone-receptor-positive, meaning estrogen fuels their growth. These women are often treated with medications like tamoxifen or aromatase inhibitors, which drastically lower estrogen levels and induce severe hot flashes. Because HRT is strictly contraindicated for these patients, non-hormonal options are essential.
The Mechanism and Efficacy: While the exact mechanism is not fully understood, it is believed that gabapentin's modulation of calcium channels in the hypothalamus helps stabilize the thermoregulatory center. Clinical trials have shown that gabapentin (typically dosed at 900 mg per day, often taken primarily at night) can reduce the frequency and severity of hot flashes by 45% to 50%, making it one of the most effective non-hormonal treatments available.
Drug Interactions: What to Avoid
As previously noted, gabapentin's lack of hepatic metabolism makes it relatively safe regarding drug-drug interactions compared to many other medications. However, there are a few critical interactions that patients and prescribers must be aware of.
Antacids and Absorption: The most significant direct interaction involves antacids containing aluminum and magnesium (such as Maalox or Mylanta). These antacids can bind to gabapentin in the gastrointestinal tract, reducing its absorption and bioavailability by up to 20%. To prevent this, patients are advised to take gabapentin at least two hours after taking any aluminum/magnesium-based antacid.
Central Nervous System Depressants: The most dangerous interactions are pharmacodynamic rather than pharmacokinetic. Combining gabapentin with other drugs that depress the central nervous system exponentially increases the risk of severe sedation, respiratory depression, and death. This includes:
- Opioids: (e.g., hydrocodone, oxycodone, morphine, fentanyl). This is the most lethal combination and the subject of the 2019 FDA Black Box Warning.
- Benzodiazepines: (e.g., alprazolam, diazepam, lorazepam).
- Alcohol: Consuming alcohol while taking gabapentin significantly impairs motor skills, cognition, and breathing.
- Muscle Relaxants and Sleep Aids: (e.g., cyclobenzaprine, zolpidem).
The History and Development of Gabapentin
The story of gabapentin's development is a fascinating journey from a theoretical chemical concept to a blockbuster drug with a vastly different clinical profile than originally intended.
The GABA Hypothesis: In the 1970s, researchers at Parke-Davis (which later became part of Pfizer) were searching for new antiepileptic drugs. They knew that the neurotransmitter GABA was the brain's primary inhibitory signal, calming electrical activity. However, pure GABA cannot cross the blood-brain barrier. The chemists designed gabapentin by taking a GABA molecule and attaching a lipophilic (fat-loving) cyclohexane ring to it, theorizing that this would allow it to cross into the brain and act directly on GABA receptors to stop seizures.
The Mechanism Surprise: The drug was synthesized, and it successfully crossed the blood-brain barrier and stopped seizures in animal models. It was approved by the FDA in 1993 as Neurontin. However, years later, advanced pharmacological studies revealed a stunning fact: gabapentin did not bind to GABA receptors at all. It had absolutely no direct effect on GABA. Instead, researchers discovered its true target: the α2δ subunit of the voltage-gated calcium channels. The drug worked brilliantly, but for entirely different reasons than its creators had designed it for.
The Off-Label Explosion: Following its approval for epilepsy, doctors began noticing that patients taking Neurontin were reporting significant relief from various types of nerve pain. This led to clinical trials for postherpetic neuralgia, securing its second FDA approval. Subsequently, aggressive (and highly controversial) marketing campaigns by the manufacturer promoted the drug for dozens of off-label uses, leading to massive legal settlements but also cementing gabapentin's place as one of the most widely prescribed drugs in modern medicine.
Neurontin Quick View
| Active Ingredient | Gabapentin |
|---|---|
| Drug Class | Gabapentinoid / Anticonvulsant |
| Fda Approved | 1993 |
| Prescription Required | 1 |
| Controlled Substance | Schedule V in some US states; Unscheduled federally |
| Half Life | 5 to 7 hours |
| Onset Of Action | 1 to 3 hours (peak plasma concentration) |
| Bioavailability | Inversely proportional to dose (e.g., 60% at 300mg, 34% at 800mg) |
| Metabolism | Not metabolized; excreted unchanged in urine |
| Pregnancy Category | Category C |
Neurontin Side Effects
Common Side Effects
- Dizziness and unsteadiness
- Somnolence (drowsiness)
- Peripheral edema (swelling in extremities)
- Fatigue and weakness
- Ataxia (loss of coordination)
Uncommon Side Effects
- Weight gain
- Tremor
- Diplopia (double vision)
- Memory impairment or 'brain fog'
- Dry mouth
Rare Side Effects
- Severe respiratory depression
- Suicidal ideation or behavior
- DRESS syndrome (severe allergic reaction)
- Anaphylaxis
- Status epilepticus (if stopped abruptly)
Important Warning: FDA Black Box Warning: Gabapentinoids can cause life-threatening respiratory depression, especially when combined with opioids, other CNS depressants, or in patients with underlying respiratory impairment. Never stop taking gabapentin abruptly due to the risk of severe withdrawal and seizures.
More Information About Neurontin
Storage
Store at room temperature between 68°F and 77°F (20°C to 25°C). Keep away from light and moisture. Do not store in the bathroom. Liquid formulations should be refrigerated.
Contraindications
Drug Interactions
Avoid taking aluminum or magnesium-based antacids within 2 hours of gabapentin. Severe, potentially fatal interactions occur when combined with opioids, benzodiazepines, alcohol, or other CNS depressants.
Neurontin FAQs
No, gabapentin is neither a narcotic nor an opioid. It is an anticonvulsant and nerve pain medication. However, it can enhance the effects of opioids, which is why the combination is dangerous and closely monitored.
Gabapentin has a relatively short half-life (5-7 hours) and its absorption in the gut is limited. Taking it three times a day ensures stable levels in your bloodstream to provide continuous pain relief or seizure control.
It is strongly advised to avoid alcohol while taking gabapentin. Both substances depress the central nervous system. Combining them significantly increases the risk of severe dizziness, drowsiness, loss of coordination, and dangerous respiratory depression.
Weight gain is a known side effect for some patients. This can be due to increased appetite or, more commonly, peripheral edema (fluid retention). If you notice sudden, significant swelling in your legs or rapid weight gain, contact your doctor.
Unlike a standard painkiller (like ibuprofen) that works immediately, gabapentin often takes 1 to 2 weeks of consistent dosing to build up in your system and provide significant relief for nerve pain.
Stopping abruptly can cause a severe withdrawal syndrome, including anxiety, insomnia, nausea, sweating, and a rapid heartbeat. In patients taking it for seizures, it can trigger life-threatening continuous seizures. Always taper off slowly under a doctor's supervision.
Written and Reviewed by Our Qualified Team

Find out more about our medical content authors and how we ensure the accuracy of our content.
Content last updated: 22 May 2026
Neurontin Reviews
Based on 25 reviews
", "It's a reliable option
", "I feel relaxed with it
Neurontin has been effective in managing my symptoms, improving my daily comfort and overall well-being. Easy to use and reliable—definitely a helpful addition to my routine.
Neurontin has been effective in managing my symptoms and improving my daily comfort. Easy to take and works well for me overall. Would recommend to others.
Neurontin has been effective in managing my symptoms and improving my daily comfort. Overall, a reliable medication that works well for me.
Neurontin has been effective for me, improving my overall well-being. It’s easy to use and fits well into my routine. Highly recommend giving it a try.
", "I've noticed improvements
", "I'm content with the outcomes
", "It promotes better days
", "Neurontin promotes well-being
", "It contributes to calm
", "Neurontin is a helpful medication
Neurontin has really helped improve my daily comfort and overall well-being. Easy to take and effective, it’s been a reliable part of my routine. Highly recommend.
Neurontin has been effective for me, providing noticeable relief and improving my overall well-being. Easy to incorporate into my routine and works as expected.
Neurontin has been effective for me, providing noticeable relief and improving my daily comfort. Easy to manage and fits well into my routine. Highly recommend.
", "It's a reliable option
", "Neurontin is helpful
", "I've found it effective
", "I'm content with performance
", "Neurontin assists routine
", "It supports my overall health
Neurontin has been effective in managing my symptoms, with noticeable improvement and good overall tolerance. I’m satisfied with the results and would recommend it.
Neurontin has been effective in managing my symptoms, with noticeable improvements. Overall, a reliable medication that fits well into my daily routine. Highly recommend.
Neurontin has been effective for me, improving my overall well-being and daily comfort. Easy to manage and noticeable results. Definitely worth considering.
Neurontin has been effective in managing my symptoms, improving my daily routine noticeably. Easy to incorporate into my schedule and overall a positive experience.
Leave a Review
How Does It Work?
Research
Read our comprehensive review to understand the medication
Consult Your Doctor
Discuss the medication with your healthcare provider
Get Your Prescription
Obtain a valid prescription from your doctor
