
Prednisone (Deltasone, Rayos)
General Health Treatment
The definitive medical guide to Prednisone: clinical applications, side effect management, tapering protocols, and comprehensive patient education.
Table of Contents
Prednisone Product Information
What is Prednisone?
Prednisone is a synthetic glucocorticoid, a type of corticosteroid medication that mimics the effects of cortisol, a hormone naturally produced by the adrenal glands. Discovered in the 1950s, it has become one of the most widely prescribed and essential medications in modern medicine due to its profound anti-inflammatory and immunosuppressive properties. Prednisone itself is a prodrug; once ingested, it is rapidly converted in the liver into its active form, prednisolone, which then exerts its therapeutic effects throughout the body.
The mechanism of action of prednisone is complex and multi-faceted. At the cellular level, the active metabolite (prednisolone) crosses the cell membrane and binds with high affinity to specific cytoplasmic glucocorticoid receptors. This receptor-steroid complex then translocates into the cell nucleus, where it binds to specific DNA sequences known as glucocorticoid response elements (GREs). This interaction alters the transcription of numerous genes. Primarily, it inhibits the synthesis of pro-inflammatory proteins (such as cytokines, chemokines, and inflammatory enzymes like COX-2) while simultaneously promoting the synthesis of anti-inflammatory proteins. The net result is a dramatic reduction in inflammation, swelling, heat, redness, and pain across various tissues and organ systems.
Furthermore, prednisone exerts potent immunosuppressive effects. It alters the function and distribution of white blood cells, particularly lymphocytes and macrophages, reducing their ability to migrate to sites of inflammation and blunting their response to antigens. This makes prednisone an invaluable tool in managing autoimmune diseases, where the body's immune system mistakenly attacks its own tissues, and in preventing organ rejection following transplantation.
Prednisone is typically administered orally in tablet or liquid form. It is readily absorbed from the gastrointestinal tract, with peak plasma concentrations occurring within one to two hours. While its half-life in the blood is relatively short (about 2 to 3 hours), its biological effects at the tissue level persist much longer, typically 18 to 36 hours, allowing for once-daily dosing in many clinical scenarios. Because of its broad spectrum of activity, prednisone is considered a cornerstone therapy for a vast array of acute and chronic medical conditions.
FDA-Approved Uses and Clinical Indications
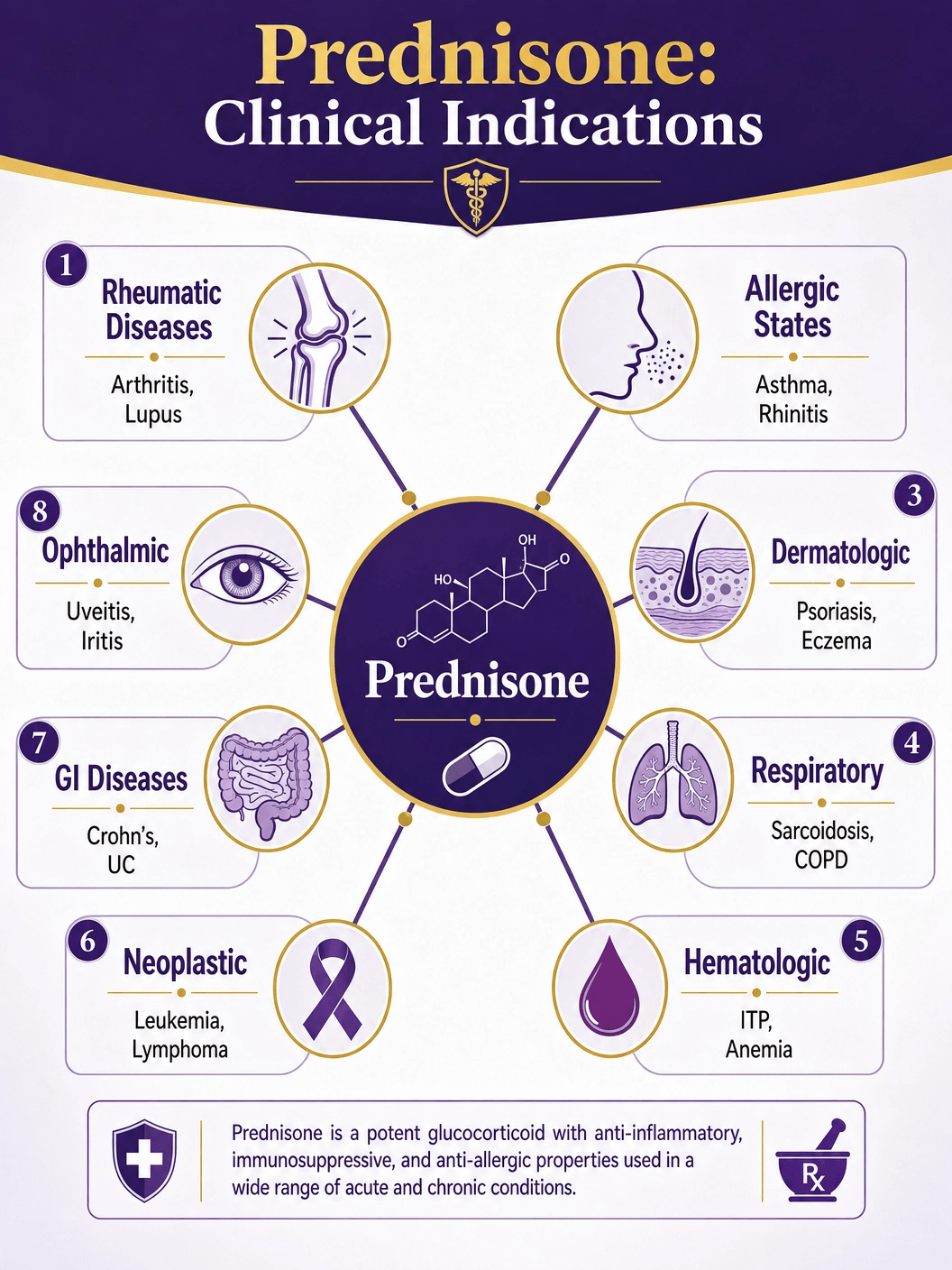
The FDA has approved prednisone for a remarkably broad spectrum of indications, spanning nearly every medical specialty. Its primary uses can be categorized into several major groups based on the underlying pathology being treated.
Endocrine Disorders: Prednisone is used as replacement therapy in conditions where the adrenal glands fail to produce sufficient natural cortisol, such as primary or secondary adrenocortical insufficiency (Addison's disease) and congenital adrenal hyperplasia. In these cases, it is often used in conjunction with a mineralocorticoid to maintain salt and water balance.
Rheumatic and Collagen Diseases: This is one of the most common applications of prednisone. It is used to manage acute exacerbations or as maintenance therapy in severe cases of rheumatoid arthritis, systemic lupus erythematosus (SLE), acute gouty arthritis, ankylosing spondylitis, and polymyalgia rheumatica. It rapidly reduces joint inflammation, pain, and stiffness, preventing long-term joint damage.
Allergic States: Prednisone is highly effective in controlling severe or incapacitating allergic conditions that do not respond to conventional treatments like antihistamines. This includes severe seasonal allergic rhinitis, bronchial asthma exacerbations, contact dermatitis (such as severe poison ivy), atopic dermatitis, serum sickness, and severe drug hypersensitivity reactions.
Dermatologic Diseases: Severe skin conditions characterized by intense inflammation or blistering are often treated with prednisone. Examples include pemphigus, severe erythema multiforme (Stevens-Johnson syndrome), exfoliative dermatitis, and severe psoriasis.
Respiratory Diseases: In pulmonology, prednisone is crucial for managing symptomatic sarcoidosis, Loeffler's syndrome, and severe asthma. It is also used in specific cases of fulminating pulmonary tuberculosis (concurrently with appropriate chemotherapy) to reduce life-threatening inflammation.
Hematologic and Neoplastic Diseases: Prednisone is used to treat autoimmune blood disorders like idiopathic thrombocytopenic purpura (ITP) and acquired hemolytic anemia. In oncology, it is a key component of palliative management and chemotherapy regimens for leukemias and lymphomas in both adults and children, often helping to induce remission and manage the side effects of other cancer treatments.
Gastrointestinal and Ophthalmic Diseases: It is used to tide patients over critical periods in inflammatory bowel diseases like ulcerative colitis and regional enteritis (Crohn's disease). In ophthalmology, it treats severe acute and chronic allergic and inflammatory processes involving the eye, such as uveitis, iritis, and optic neuritis, preventing permanent vision loss.
Understanding Side Effects and Serious Risks
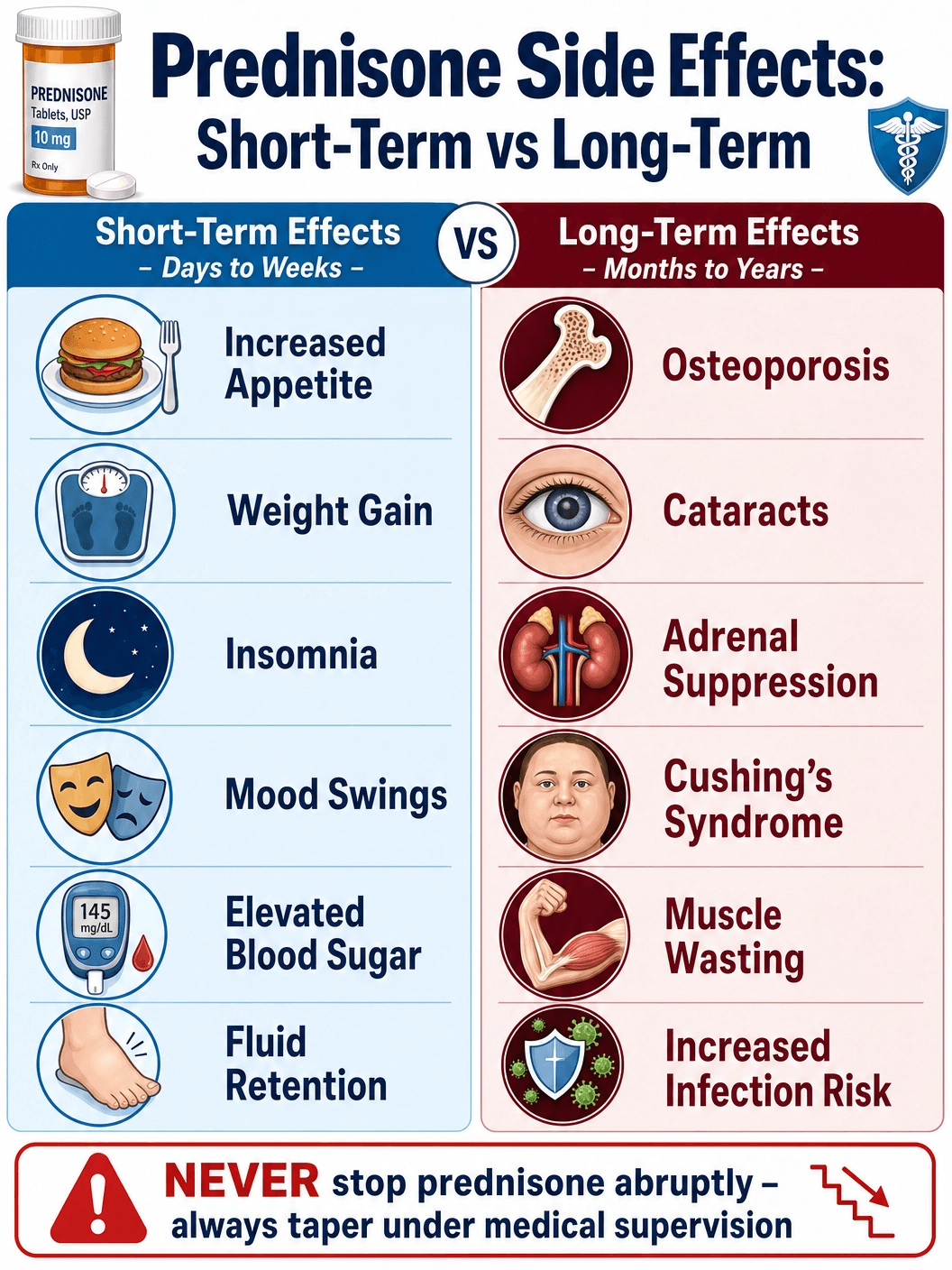
While prednisone is a highly effective and often life-saving medication, its use is associated with a wide array of potential side effects. The risk and severity of these adverse effects are directly related to the dosage and the duration of therapy. Short-term use (a few days to a couple of weeks) is generally well-tolerated, but long-term use requires careful medical supervision.
Short-Term Side Effects: Even with brief courses of prednisone, patients may experience noticeable changes. Common short-term side effects include increased appetite, weight gain, fluid retention (leading to swelling in the lower legs or hands), elevated blood pressure, and changes in mood or behavior, ranging from mild euphoria or irritability to severe anxiety and insomnia. It can also cause a temporary increase in blood sugar levels, which is particularly important for diabetic patients to monitor.
Long-Term Side Effects: Prolonged use of prednisone significantly increases the risk of more serious complications. One of the most significant concerns is osteoporosis (thinning of the bones), which increases the risk of fractures, particularly in the spine and hips. Corticosteroids decrease calcium absorption and inhibit bone formation. Patients on long-term therapy often require calcium and vitamin D supplementation, and sometimes bisphosphonate medications, to protect their bone health.
Another major long-term risk is the development of Cushing's syndrome, characterized by a redistribution of body fat (resulting in a 'moon face' and a 'buffalo hump' on the upper back), thinning of the skin, easy bruising, and poor wound healing. Long-term use also increases the risk of developing cataracts and glaucoma, necessitating regular eye examinations.
Immunosuppression and Infection Risk: Because prednisone suppresses the immune system, it significantly increases the patient's susceptibility to infections—bacterial, viral, fungal, and parasitic. It can also mask the early signs of an infection, allowing it to progress unnoticed. Patients on prednisone must be vigilant about avoiding exposure to contagious illnesses, particularly chickenpox and measles, which can be severe or even fatal in immunosuppressed individuals. Furthermore, latent infections, such as tuberculosis or amebiasis, can be reactivated during corticosteroid therapy.
Adrenal Suppression: Perhaps the most critical physiological consequence of long-term prednisone use is the suppression of the hypothalamic-pituitary-adrenal (HPA) axis. When the body receives synthetic cortisol (prednisone) from an outside source, the adrenal glands stop producing their own natural cortisol. If prednisone is stopped abruptly, the dormant adrenal glands cannot immediately resume production, leading to a potentially life-threatening condition called acute adrenal crisis. Symptoms include severe weakness, nausea, vomiting, low blood pressure, and shock. This is why prednisone must always be tapered slowly under medical supervision.
Contraindications: When Prednisone is Not Safe
Prednisone is contraindicated in patients with a known hypersensitivity or severe allergic reaction to prednisone or any of the inactive ingredients in the specific formulation. It is also strictly contraindicated in patients with systemic fungal infections, as the immunosuppressive effects of the drug can allow the infection to spread rapidly and become fatal.
While not absolute contraindications, prednisone must be used with extreme caution in several clinical scenarios. Patients with latent tuberculosis or tuberculin reactivity must be monitored closely, as prednisone can reactivate the disease; chemoprophylaxis is often required during prolonged steroid therapy. Similarly, it should be used with great care in patients with known or suspected Strongyloides (threadworm) infestation, as corticosteroid-induced immunosuppression can lead to hyperinfection and widespread larval migration.
Prednisone should be used cautiously in patients with a history of psychiatric disorders, as it can exacerbate emotional instability, depression, or psychotic tendencies. It also requires careful management in patients with gastrointestinal disorders such as active peptic ulcers, diverticulitis, or fresh intestinal anastomoses, due to an increased risk of gastrointestinal perforation and bleeding.
In pregnancy, prednisone is generally considered a Category C drug. While it has been used extensively without widespread evidence of congenital anomalies, it can cross the placenta. Infants born to mothers who received substantial doses during pregnancy must be carefully observed for signs of hypoadrenalism. The decision to use prednisone during pregnancy must weigh the potential benefits to the mother against the potential risks to the fetus. Prednisone is excreted in breast milk, so nursing mothers should consult their physician before use.
Available Dosages and Clinical Monitoring
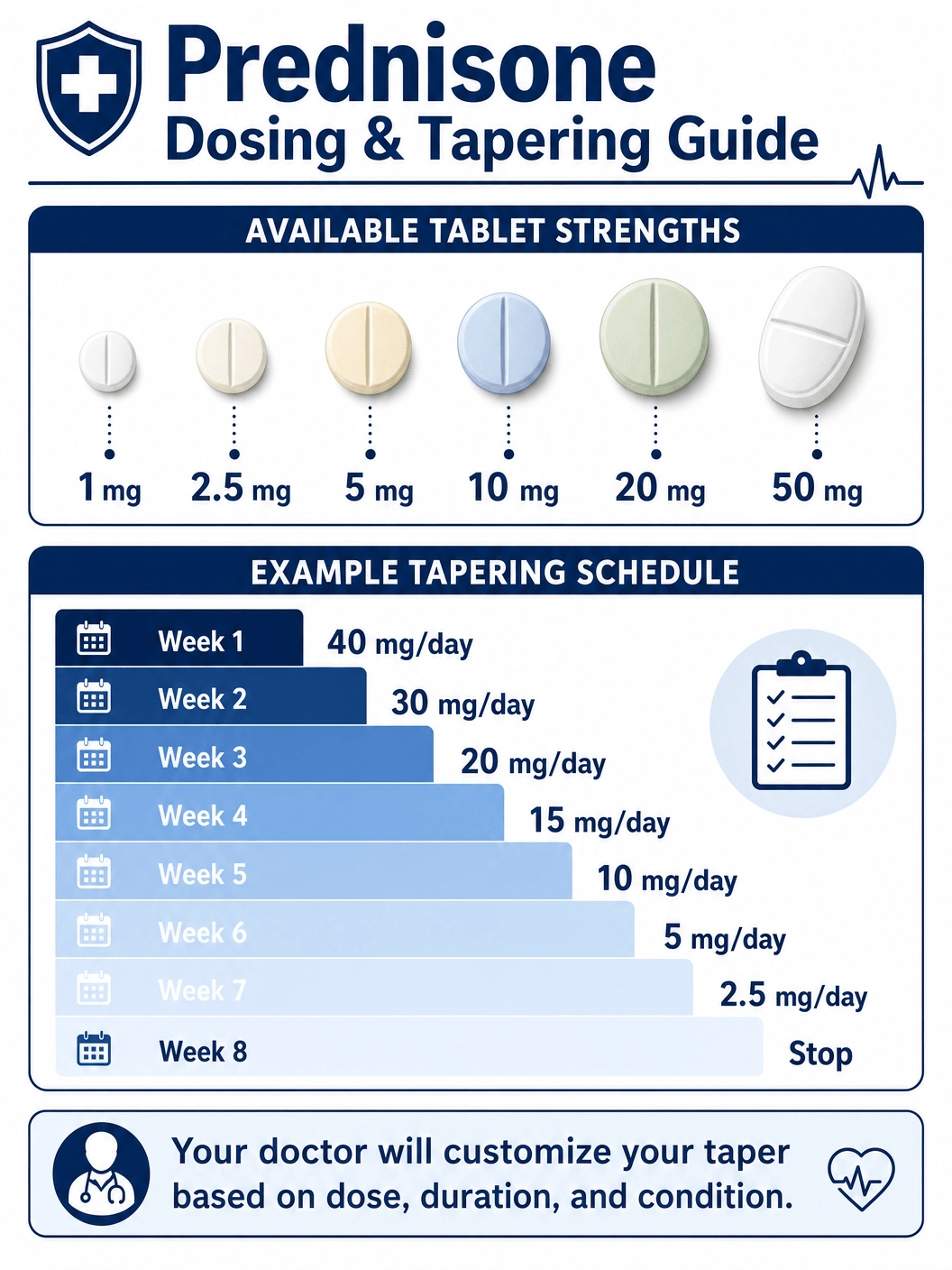
Prednisone dosing is highly variable and must be individualized based on the specific disease being treated, its severity, and the patient's response. The goal of therapy is always to use the lowest effective dose for the shortest possible duration to minimize adverse effects.
Low to Moderate Doses (1mg to 20mg)
Prednisone is available in a wide range of tablet strengths, including 1 mg, 2.5 mg, 5 mg, 10 mg, and 20 mg. Low doses (typically 1 to 10 mg per day) are often used for maintenance therapy in chronic autoimmune conditions like rheumatoid arthritis or systemic lupus erythematosus, aiming to keep inflammation at bay while minimizing long-term side effects. Moderate doses (10 to 20 mg per day) might be used for less severe acute flare-ups of inflammatory conditions or as a step-down dose during a tapering schedule.
High Doses (50mg and Above)
For severe, acute, or life-threatening conditions—such as a severe asthma attack, acute rejection of a transplanted organ, severe allergic reactions, or the initial management of certain leukemias—high doses of prednisone are required. The 50 mg tablet is often utilized in these scenarios. Initial dosages can range from 5 mg to 60 mg or more per day. In some critical situations, massive doses (e.g., 100 mg to 250 mg daily) may be administered for a short period to rapidly suppress the immune response and halt tissue damage.
The Importance of Tapering
Regardless of the initial dose, if prednisone has been taken for more than a few weeks, it must never be stopped abruptly. Because the drug suppresses the body's natural production of cortisol, a sudden cessation can trigger an adrenal crisis. To prevent this, physicians employ a tapering schedule, gradually reducing the dose over days, weeks, or even months, depending on how long the patient has been on the medication. This slow reduction allows the adrenal glands time to 'wake up' and resume their normal function. The specific tapering schedule is highly individualized and must be strictly followed by the patient.
Generic vs. Brand Name Prednisone
Prednisone is widely available as a generic medication, which is the most common way it is prescribed and dispensed. However, several brand-name formulations exist, offering specific delivery mechanisms or historical familiarity.
Generic Prednisone: Generic prednisone tablets are manufactured by numerous pharmaceutical companies. They are subject to strict FDA regulations requiring them to be bioequivalent to the original brand-name drugs, meaning they deliver the same amount of active ingredient into the bloodstream at the same rate. Generic prednisone is highly cost-effective and is the standard of care for the vast majority of patients requiring corticosteroid therapy.
Brand Names (Deltasone, Rayos): Deltasone was one of the original, widely recognized brand names for immediate-release prednisone, though it is less commonly dispensed today as generics dominate the market. A more recent and specialized brand-name formulation is Rayos. Rayos is a delayed-release prednisone tablet. It is designed to be taken at bedtime; the tablet's coating delays the release of the medication for about four hours. This timing is specifically engineered for conditions like rheumatoid arthritis, where inflammatory cytokines peak during the early morning hours, causing severe morning stiffness. By delaying the release, Rayos aims to deliver peak drug concentrations exactly when the inflammation is highest. However, Rayos is significantly more expensive than generic immediate-release prednisone.
For most patients, generic immediate-release prednisone is perfectly adequate and much more affordable. The choice between generic and a specialized brand like Rayos should be made in consultation with a rheumatologist or primary care physician, weighing the specific clinical needs against the cost.
Purchasing Prednisone: Cost and Legal Acquisition
Prednisone is a relatively inexpensive medication, particularly when purchased in its generic form. Without insurance, a typical short-term prescription (e.g., a dose pack or a two-week supply) of generic prednisone usually costs between $10 and $20 at most major pharmacies. For patients on long-term maintenance therapy, a month's supply of generic tablets remains highly affordable, often under $15. Brand-name formulations like Rayos, however, can cost hundreds or even thousands of dollars per month and often require specific insurance authorization.
Legal Acquisition: Prednisone is a prescription-only medication in the United States and most other countries. It cannot be legally purchased over the counter. Because of its profound effects on the immune and endocrine systems, and the significant risks associated with improper use or abrupt discontinuation, it must be prescribed by a licensed healthcare provider following a thorough medical evaluation. Patients should only obtain prednisone from reputable, licensed pharmacies to ensure they are receiving the correct dosage and a safe, unadulterated product.
Official Instructions and Guidelines
To maximize the benefits of prednisone while minimizing its risks, patients must adhere strictly to the prescribing instructions provided by their healthcare professional.
Administration: Prednisone should always be taken with food or milk to reduce the risk of gastrointestinal irritation and stomach upset, which are common side effects. If you are prescribed a once-daily dose, it is generally recommended to take it in the morning (usually before 9:00 AM). This timing mimics the body's natural diurnal rhythm of cortisol production, which peaks in the early morning, thereby helping to minimize the suppression of the adrenal glands and reducing the risk of insomnia.
Missed Doses: If you miss a dose of prednisone, take it as soon as you remember. However, if it is almost time for your next scheduled dose, skip the missed dose and resume your regular dosing schedule. Do not double the dose to catch up, as this can increase the risk of side effects. If you are on an alternate-day dosing schedule and miss a dose, contact your doctor for specific instructions.
Medical Identification: Patients taking prednisone for a prolonged period should carry a medical identification card or wear a medical alert bracelet stating that they are on corticosteroid therapy. In the event of a medical emergency, trauma, or severe illness, healthcare providers need to know this information immediately, as the patient may require supplemental 'stress doses' of steroids to help their body cope with the physical stress, since their own adrenal glands are suppressed.
When to Call Your Doctor
While on prednisone therapy, vigilant monitoring of your health is crucial. You should contact your doctor promptly if you experience any of the following:
- Signs of Infection: Because prednisone suppresses the immune system, report any signs of infection immediately, including fever, chills, persistent sore throat, cough, or pain during urination. Do not assume it is just a minor cold.
- Severe Mood Changes: If you experience severe depression, extreme mood swings, hallucinations, or thoughts of self-harm, seek medical attention immediately.
- Gastrointestinal Issues: Report severe abdominal pain, or black, tarry stools, which could indicate a bleeding ulcer.
- Vision Changes: Any blurred vision, eye pain, or seeing halos around lights should be evaluated by an eye specialist, as these could be signs of increased intraocular pressure or cataracts.
- Signs of Adrenal Insufficiency: If you are tapering off the medication and experience severe fatigue, weakness, nausea, vomiting, or dizziness (especially upon standing), contact your doctor immediately, as your taper may need to be adjusted.
Government and Regulatory Resources
For authoritative, up-to-date information regarding Prednisone, its approved uses, safety warnings, and clinical guidelines, please consult the following resources:
- DailyMed: Prednisone Tablet Label - Comprehensive prescribing information provided by the National Library of Medicine.
- NCBI StatPearls: Prednisone Overview - A detailed clinical overview of prednisone, its mechanism, and adverse effects.
- FDA Prescribing Information for Rayos (Delayed-Release Prednisone) - Specific label information for the delayed-release formulation.
- Cleveland Clinic: Prednisone Tablets - Patient-friendly information on uses, side effects, and precautions.
Editorial Review & Medical Sources
This guide is for informational purposes and does not constitute medical advice. Content is based on clinical data from the FDA, the National Institutes of Health (NIH), and the Cleveland Clinic. Medical Reviewer: Dr. Sanjai Sinha, MD. Primary Sources: FDA Prescribing Information, StatPearls Clinical Database (NCBI).
Prednisone vs. Prednisolone: Understanding the Difference
Patients and even some healthcare providers often use the terms prednisone and prednisolone interchangeably, but there is a distinct and clinically important difference between the two medications. Understanding this difference is crucial, particularly for patients with specific underlying health conditions.
The Prodrug Concept: As mentioned earlier, prednisone is a prodrug. This means that in its original form, as it exists in the tablet you swallow, it is biologically inactive. It cannot bind to glucocorticoid receptors or reduce inflammation on its own. For prednisone to work, it must first pass through the liver. In the liver, an enzyme called 11-beta-hydroxysteroid dehydrogenase type 1 (11-beta-HSD1) chemically converts the inactive prednisone into the active molecule, prednisolone. It is this newly formed prednisolone that then circulates through the bloodstream and exerts the powerful anti-inflammatory and immunosuppressive effects.
Prednisolone as a Direct Medication: Prednisolone, on the other hand, is already in its active form. When a patient takes a prednisolone tablet or liquid, it does not need to be processed by the liver to become effective; it is ready to bind to receptors immediately upon absorption into the bloodstream.
Clinical Implications: For the vast majority of patients with healthy liver function, the difference between taking prednisone and prednisolone is negligible. The liver rapidly and efficiently converts prednisone to prednisolone, and the clinical outcomes are identical. Therefore, prednisone is usually the default prescription because it is often slightly cheaper and more widely available in various tablet strengths.
However, the distinction becomes critical in patients with severe liver disease, such as advanced cirrhosis or severe hepatitis. In these individuals, the liver's enzymatic machinery may be impaired, meaning it cannot efficiently convert the inactive prednisone into the active prednisolone. If such a patient is given prednisone, they may not receive the intended therapeutic benefit because the drug remains largely inactive in their system. For patients with significant hepatic impairment, prescribing prednisolone directly is the safer and more effective choice, ensuring they receive the active medication without relying on compromised liver function.
Managing the Psychological and Emotional Side Effects
While the physical side effects of prednisone—like weight gain and osteoporosis—are well-documented and frequently discussed, the psychological and emotional impacts are often under-recognized, yet they can be profoundly distressing for patients. Corticosteroids can significantly alter mood, behavior, and cognitive function, a phenomenon sometimes referred to as 'steroid psychosis' in severe cases, though milder mood disturbances are much more common.
The Spectrum of Mood Changes: The psychological effects of prednisone are highly variable and unpredictable. Some patients experience a mild, almost pleasant euphoria or increased energy levels, particularly when starting the medication. However, this can quickly shift to irritability, agitation, and severe anxiety. Patients often report feeling 'wired,' jittery, or unable to relax, which frequently contributes to severe insomnia. The lack of sleep then exacerbates the irritability and emotional lability.
In more severe cases, prednisone can trigger profound depression, crying spells, and a sense of hopelessness. At the extreme end of the spectrum, high doses can induce manic episodes, delirium, and frank psychosis, characterized by hallucinations (seeing or hearing things that aren't there) and delusions (false beliefs). These severe psychiatric reactions are more common at higher doses (typically above 40 mg per day) but can occur at any dose.
Coping Strategies and Medical Management: It is vital for patients and their families to be aware that these mood changes are a chemical side effect of the medication, not a personal failing or a permanent psychological condition. If you experience significant mood swings, anxiety, or depression while on prednisone, you must communicate this to your prescribing doctor immediately.
Management strategies may include:
- Dosage Adjustment: The most effective way to resolve steroid-induced mood changes is to lower the dose of prednisone, if the underlying medical condition allows for it. This must always be done via a medically supervised taper.
- Timing of Doses: Taking the entire daily dose in the morning can sometimes help mitigate insomnia, which in turn can improve overall mood and emotional resilience.
- Adjunctive Medications: In cases where the prednisone dose cannot be lowered, doctors may prescribe medications to manage the psychiatric symptoms. This might include sleep aids for insomnia, anti-anxiety medications, or, in severe cases of steroid psychosis, antipsychotic medications or mood stabilizers.
- Support Systems: Open communication with family members about the potential for mood changes is crucial so they can provide support and understanding rather than reacting to the irritability.
Dietary Considerations While on Prednisone
Because prednisone significantly alters the body's metabolism, paying close attention to your diet is a critical component of managing the medication's side effects and maintaining overall health during therapy. Prednisone affects how the body processes carbohydrates, proteins, fats, sodium, and calcium.
Managing Blood Sugar and Weight: Prednisone promotes gluconeogenesis (the production of glucose by the liver) and decreases the cellular uptake of glucose, leading to elevated blood sugar levels. It also dramatically increases appetite. This combination frequently results in rapid weight gain and, in some cases, steroid-induced diabetes. To combat this, patients should focus on a diet low in simple, refined carbohydrates (like sugary drinks, candies, and white bread) and high in complex carbohydrates (like whole grains, legumes, and vegetables) which cause a slower, steadier rise in blood sugar. Portion control is essential to manage the increased appetite.
Sodium and Fluid Retention: Corticosteroids cause the kidneys to retain sodium and excrete potassium. The retained sodium pulls water with it, leading to fluid retention, swelling (edema), and increased blood pressure. A strict low-sodium diet is highly recommended. This means avoiding processed foods, canned soups, fast food, and adding extra salt to meals. Instead, flavor food with herbs and spices. Concurrently, increasing the intake of potassium-rich foods—such as bananas, oranges, spinach, and tomatoes—can help counteract the potassium loss.
Protecting Bone Health: As prednisone inhibits calcium absorption in the gut and increases its excretion in the urine, it directly contributes to bone loss and osteoporosis. A diet rich in calcium and Vitamin D is imperative. Good sources of calcium include dairy products (milk, yogurt, cheese), leafy green vegetables (kale, collard greens), and fortified plant-based milks. Vitamin D, which is necessary for calcium absorption, can be obtained from fortified foods, fatty fish, and safe sun exposure. In many cases, dietary intake alone is insufficient, and doctors will recommend calcium and Vitamin D supplements to protect bone density during long-term prednisone therapy.
Protein Intake: Prednisone can cause muscle wasting (myopathy) by breaking down proteins in the muscles. Ensuring an adequate intake of high-quality, lean protein—such as poultry, fish, eggs, beans, and tofu—can help mitigate this muscle loss and support tissue repair.
Drug Interactions: A Comprehensive Overview
Prednisone interacts with a significant number of other medications, supplements, and even certain foods. These interactions can either reduce the effectiveness of prednisone, increase the risk of its side effects, or alter the effects of the other medications being taken concurrently. Patients must always provide their healthcare provider with a complete list of all medications, supplements, and herbal products they are taking before starting prednisone therapy.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): The combination of prednisone with NSAIDs such as ibuprofen (Advil, Motrin), naproxen (Aleve), or aspirin significantly increases the risk of gastrointestinal ulceration and bleeding. Both drug classes independently irritate the stomach lining and inhibit its protective mechanisms. When used together, the risk of developing a peptic ulcer or experiencing a serious gastrointestinal hemorrhage is substantially elevated. If concurrent use is unavoidable, a proton pump inhibitor (PPI) such as omeprazole may be prescribed to protect the stomach lining.
Diabetes Medications: Prednisone raises blood glucose levels by promoting gluconeogenesis and reducing insulin sensitivity. This directly counteracts the effects of diabetes medications, including insulin, metformin, sulfonylureas (like glipizide or glyburide), and other oral hypoglycemic agents. Diabetic patients starting prednisone therapy will almost certainly require an adjustment (increase) in their diabetes medication dosages, along with more frequent blood sugar monitoring. Some patients who were previously well-controlled may temporarily need to start insulin therapy during a prednisone course.
Blood Thinners (Anticoagulants): Prednisone can alter the effectiveness of warfarin (Coumadin) and other anticoagulants. The interaction is complex and somewhat unpredictable—it can either increase or decrease the anticoagulant effect. Patients on warfarin who start or stop prednisone must have their INR (International Normalized Ratio) monitored more frequently to ensure their blood-thinning level remains in the safe therapeutic range and to prevent either dangerous bleeding or clotting.
Live Vaccines: Patients taking immunosuppressive doses of prednisone must not receive live or live-attenuated vaccines. Because prednisone suppresses the immune system, a live vaccine—which contains a weakened but living form of the virus or bacteria—could potentially cause the very infection it is meant to prevent. Examples of live vaccines include MMR (measles, mumps, rubella), varicella (chickenpox), oral polio, yellow fever, and the nasal spray influenza vaccine. Inactivated vaccines (like the flu shot or COVID-19 mRNA vaccines) are generally safe but may produce a weaker immune response in patients on prednisone.
CYP3A4 Enzyme Interactions: Prednisone is metabolized in the liver by the cytochrome P450 enzyme system, particularly the CYP3A4 enzyme. Drugs that inhibit this enzyme—such as ketoconazole (an antifungal), ritonavir (an HIV protease inhibitor), and grapefruit juice—can slow the breakdown of prednisone, effectively increasing its levels in the body and raising the risk of side effects. Conversely, drugs that induce (speed up) CYP3A4—such as rifampin (an antibiotic for tuberculosis), phenytoin (an anti-seizure medication), and barbiturates—can accelerate the metabolism of prednisone, reducing its effectiveness and potentially requiring a dose increase.
Diuretics and Potassium: Prednisone causes the kidneys to retain sodium and excrete potassium. When combined with potassium-wasting diuretics (such as furosemide or hydrochlorothiazide), the risk of dangerously low potassium levels (hypokalemia) is significantly increased. Hypokalemia can cause muscle weakness, cramps, irregular heartbeat, and in severe cases, cardiac arrest. Potassium levels should be monitored regularly, and supplementation may be necessary.
Cardiac Glycosides (Digoxin): The hypokalemia caused by prednisone can increase the toxicity of digoxin, a medication used to treat heart failure and certain arrhythmias. Low potassium levels make the heart more sensitive to digoxin's effects, potentially leading to dangerous cardiac arrhythmias. Close monitoring of both potassium levels and digoxin levels is essential when these medications are used together.
Prednisone Use in Children and Adolescents
Prednisone is frequently prescribed to children for a variety of conditions, including severe asthma, nephrotic syndrome, inflammatory bowel disease, juvenile idiopathic arthritis, and certain cancers like acute lymphoblastic leukemia (ALL). While it is often essential and life-saving in pediatric populations, its use in growing children carries unique risks that require careful consideration and monitoring.
Growth Suppression: One of the most significant concerns with long-term prednisone use in children is its effect on linear growth. Corticosteroids can suppress the growth hormone axis and directly inhibit the growth plates (epiphyseal plates) in bones. Children on prolonged prednisone therapy may experience a slowing or temporary cessation of growth. The degree of growth suppression depends on the dose, duration, and the child's age. In many cases, growth velocity recovers after the medication is discontinued or reduced, but some children may not fully catch up to their predicted adult height if the suppression was prolonged or occurred during critical growth periods.
Alternate-Day Dosing: To mitigate the impact on growth and other long-term side effects, pediatricians often employ an alternate-day dosing strategy when possible. Instead of taking prednisone every day, the child takes a double dose every other day. This approach allows the HPA axis to partially recover on the 'off' days, reducing the degree of adrenal suppression and potentially lessening the impact on growth. However, alternate-day dosing is not appropriate for all conditions—some diseases require daily suppression to maintain control.
Behavioral and Emotional Effects in Children: Children and adolescents may be particularly susceptible to the mood-altering effects of prednisone. Parents and caregivers should be aware that children on prednisone may exhibit increased irritability, hyperactivity, emotional lability (rapid mood swings), aggression, or difficulty concentrating. These behavioral changes can be distressing for both the child and the family, and can sometimes be mistaken for behavioral disorders. It is important for parents to understand that these are pharmacological effects of the medication and will typically resolve once the dose is reduced or the medication is discontinued.
Monitoring in Pediatric Patients: Children on long-term prednisone therapy require regular monitoring that goes beyond what is typically needed for adults. This includes periodic measurements of height and weight plotted on growth charts, bone density assessments (DEXA scans) in children on prolonged therapy, regular eye examinations to screen for cataracts and glaucoma, blood pressure monitoring, and periodic blood tests to check glucose levels, electrolytes, and adrenal function. Vaccinations must be carefully managed—live vaccines are contraindicated during immunosuppressive therapy, and the timing of routine childhood immunizations may need to be adjusted.
Prednisone in Elderly Patients: Special Considerations
Elderly patients represent another population requiring special attention when prednisone is prescribed. Age-related physiological changes alter both the pharmacokinetics (how the body processes the drug) and the pharmacodynamics (how the drug affects the body) of prednisone, and older adults are more vulnerable to many of its adverse effects.
Increased Osteoporosis Risk: Older adults, particularly postmenopausal women, already have an elevated baseline risk of osteoporosis due to age-related bone loss and declining estrogen levels. Adding prednisone to this equation dramatically accelerates bone loss. Studies have shown that corticosteroid-induced osteoporosis can lead to vertebral compression fractures in as many as 30-50% of patients on long-term therapy. For elderly patients starting prednisone, a baseline DEXA scan is strongly recommended, along with aggressive preventive measures including calcium (1000-1200 mg/day), vitamin D (800-1000 IU/day), and often a bisphosphonate medication (such as alendronate) to protect bone density.
Increased Infection Susceptibility: The aging immune system (a phenomenon known as immunosenescence) is already less robust in fighting infections. When prednisone further suppresses this already-weakened immune system, elderly patients become extremely vulnerable to infections. Pneumonia, urinary tract infections, and skin infections can develop more easily and progress more rapidly. Reactivation of latent herpes zoster (shingles) is also more common in immunosuppressed elderly patients.
Cardiovascular and Metabolic Risks: Elderly patients are more likely to have pre-existing cardiovascular disease, hypertension, and diabetes—all of which can be worsened by prednisone. The fluid retention and sodium retention caused by prednisone can exacerbate heart failure. The hyperglycemic effects can destabilize previously well-controlled diabetes. Blood pressure may rise significantly. These patients require more frequent monitoring of blood pressure, blood glucose, weight, and signs of fluid overload.
Cognitive Effects and Delirium: Older adults are more susceptible to the neuropsychiatric effects of corticosteroids. While younger patients might experience mood swings or insomnia, elderly patients—particularly those with pre-existing cognitive impairment—may develop confusion, disorientation, or frank delirium. This is especially common in hospitalized elderly patients receiving high-dose corticosteroids. Healthcare providers should use the lowest effective dose and monitor cognitive function closely.
The History of Corticosteroids: From Discovery to Modern Medicine
The story of prednisone and corticosteroids is one of the most remarkable chapters in the history of modern pharmacology. It begins in the early twentieth century with the recognition that the adrenal glands produced substances essential for life, and culminates in a Nobel Prize and the development of medications that have saved countless lives.
Early Discoveries (1930s-1940s): In the 1930s, researchers including Edward Calvin Kendall at the Mayo Clinic and Tadeus Reichstein in Switzerland independently isolated several hormones from the adrenal cortex. These were initially designated as Compounds A through F. Compound E, later named cortisone, proved to be of particular interest due to its biological activity. However, isolating sufficient quantities for clinical use was extraordinarily difficult—it required processing tons of animal adrenal glands to obtain tiny amounts of the pure hormone.
The Breakthrough (1948-1950): The pivotal moment came in 1948 when Philip Hench, a rheumatologist at the Mayo Clinic, administered cortisone to a patient with severe, crippling rheumatoid arthritis. The results were nothing short of miraculous—within days, the patient, who had been bedridden and in excruciating pain, was able to walk and move freely. This dramatic demonstration electrified the medical world. In 1950, Hench, Kendall, and Reichstein were awarded the Nobel Prize in Physiology or Medicine for their discoveries relating to the hormones of the adrenal cortex.
The Development of Synthetic Analogs (1950s): While cortisone was revolutionary, it had significant limitations—particularly its strong mineralocorticoid effects (causing salt and water retention). Pharmaceutical chemists set about modifying the cortisone molecule to create synthetic analogs with enhanced anti-inflammatory potency but reduced mineralocorticoid side effects. Prednisone was introduced in 1955 as one of these improved synthetic glucocorticoids. It offered approximately four times the anti-inflammatory potency of cortisone with significantly less sodium retention, making it more suitable for long-term therapeutic use.
Modern Era: Since its introduction nearly seven decades ago, prednisone has remained one of the most prescribed medications worldwide. It appears on the World Health Organization's List of Essential Medicines—a catalog of the most important medications needed in a basic health system. While newer, more targeted therapies (such as biologics for autoimmune diseases) have reduced the reliance on corticosteroids in some conditions, prednisone remains irreplaceable for many acute and chronic medical situations due to its broad efficacy, rapid onset, oral availability, and extremely low cost.
Lifestyle Modifications and Supportive Care During Prednisone Therapy
Beyond dietary changes, patients on prednisone therapy—particularly those on long-term courses—should adopt several lifestyle modifications to counteract the medication's adverse effects and maintain the best possible quality of life.
Exercise and Physical Activity: Regular weight-bearing and resistance exercise is one of the most effective non-pharmacological strategies for combating prednisone-induced osteoporosis and muscle wasting. Activities such as walking, jogging, climbing stairs, dancing, and lifting light weights stimulate bone formation and help maintain muscle mass and strength. Exercise also helps manage weight gain, improves mood (counteracting steroid-induced depression and anxiety), enhances sleep quality, and helps regulate blood sugar levels. Patients should aim for at least 30 minutes of moderate exercise most days of the week, adapting the intensity to their physical capabilities and underlying medical condition.
Sleep Hygiene: Insomnia is one of the most common and distressing side effects of prednisone. Patients can improve their sleep by practicing good sleep hygiene: maintaining a consistent sleep-wake schedule, avoiding caffeine and stimulating activities in the evening, keeping the bedroom cool and dark, limiting screen time before bed, and using relaxation techniques such as deep breathing or meditation. Taking the prednisone dose in the morning (rather than later in the day) can also help, as the stimulating effects will have diminished somewhat by bedtime.
Skin Care: Prednisone thins the skin and makes it more fragile and prone to bruising, tearing, and poor wound healing. Patients should take extra care to protect their skin: using gentle, fragrance-free moisturizers regularly, avoiding harsh soaps, wearing protective clothing when gardening or doing activities that could cause skin injuries, and using sunscreen to protect against sun damage (which is amplified by thin skin). Any wounds or cuts should be cleaned and monitored carefully for signs of infection, as healing will be slower.
Mental Health Support: Given the significant psychological effects of prednisone, patients on long-term therapy should not hesitate to seek mental health support. This might include regular check-ins with a therapist or counselor, joining a support group for people on chronic corticosteroid therapy, practicing mindfulness or meditation, and maintaining strong social connections. Family members should be educated about the potential mood effects so they can provide understanding and support rather than taking behavioral changes personally.
Infection Prevention: Because prednisone weakens the immune system, patients should take proactive steps to reduce their exposure to infections. This includes frequent handwashing, avoiding crowded places during flu season, staying up to date on recommended inactivated vaccines (such as the annual flu shot and pneumococcal vaccine), avoiding contact with people who are actively ill, and practicing food safety to prevent foodborne infections. Any signs of infection—even seemingly minor ones—should be reported to a healthcare provider promptly.
Prednisone Quick View
| Active Ingredient | Prednisone (converted to Prednisolone in liver) |
|---|---|
| Manufacturer | Various Generics |
| Type | Glucocorticoid / Immunosuppressant |
| Onset | Peak plasma concentration in 1-2 hours |
| Duration | Biological half-life 18-36 hours |
| Food Interaction | Take with food or milk to prevent stomach upset |
| Alcohol | Avoid; increases risk of stomach ulcers and bleeding |
| Prescription | Required |
Prednisone Side Effects
Common Side Effects
- Increased appetite and weight gain.
- Fluid retention and swelling (edema).
- Mood changes, irritability, or insomnia.
- Elevated blood sugar levels.
- Stomach upset or indigestion.
Uncommon Side Effects
- High blood pressure.
- Muscle weakness (myopathy).
- Thinning of the skin and easy bruising.
- Increased susceptibility to infections.
Rare Side Effects
- Osteoporosis and bone fractures (with long-term use).
- Cataracts or glaucoma.
- Adrenal suppression and crisis (if stopped abruptly).
- Steroid psychosis (severe mood or behavioral changes).
Important Warning: CRITICAL SAFETY WARNING: Never stop taking prednisone abruptly if you have been on it for more than a few weeks. A gradual taper is required to prevent life-threatening adrenal crisis.
More Information About Prednisone
Storage
Store at room temperature between 15 and 30 degrees C (59 and 86 degrees F). Protect from light and moisture.
Contraindications
Contraindicated in patients with systemic fungal infections or known hypersensitivity. Use with extreme caution in patients with latent tuberculosis, active peptic ulcers, or psychiatric disorders.
Drug Interactions
Interacts with NSAIDs (increases ulcer risk), diabetes medications (may require dose adjustment), vaccines (live vaccines contraindicated), and blood thinners.
Prednisone FAQs
Prednisone stops your adrenal glands from making natural cortisol. Tapering slowly gives your glands time to 'wake up' and start producing cortisol again, preventing a dangerous adrenal crisis.
Prednisone is inactive until your liver converts it into prednisolone. For most people, they work the same. However, people with severe liver disease should take prednisolone directly.
Prednisone increases appetite and changes metabolism. Focus on a low-sodium, low-sugar diet rich in lean proteins and complex carbohydrates, and practice strict portion control.
It is best to avoid alcohol. Both alcohol and prednisone can irritate the stomach lining, and combining them significantly increases the risk of developing stomach ulcers or gastrointestinal bleeding.
Prednisone is absorbed quickly and reaches peak blood levels within 1-2 hours. Most patients notice some improvement in inflammation within a few hours, though the full therapeutic effect may take 1-3 days.
Yes. Prednisone can cause mood swings, irritability, anxiety, euphoria, insomnia, and in rare cases, severe depression or psychosis. These effects are dose-dependent and typically resolve when the medication is tapered.
Written and Reviewed by Our Qualified Team

Find out more about our medical content authors and how we ensure the accuracy of our content.
Content last updated: 21 May 2026
Prednisone Reviews
Based on 43 reviews
Excellent results with Prednisone! It quickly brought my flare-up under control. I appreciate the quick action of Prednisone when I need immediate relief.
Prednisone is a vital medication for many, and I'm thankful for its existence.
Prednisone is a vital medication for many, and I'm thankful for its existence. Prednisone made me feel very irritable and short-tempered. Not pleasant for anyone around me.
I've had some stomach issues and heartburn since starting Prednisone. It's uncomfortable. It's important to follow the dosage instructions for Prednisone carefully to minimize side effects.
Prednisone made me feel very irritable and short-tempered. Not pleasant for anyone around me. Prednisone is a vital medication for many, and I'm thankful for its existence.
I've learned to anticipate some of the side effects of Prednisone and manage them.
I've been taking Prednisone for a while now, and it really helps manage my symptoms. Feeling much better.
It's important to follow the dosage instructions for Prednisone carefully to minimize side effects. Prednisone is a strong medication, but it's been very effective in treating my lupus symptoms.
I'm impressed with how quickly Prednisone alleviated my severe rash. It's a powerful steroid. However, While Prednisone is effective, the side effects are quite challenging. I've experienced mood swings.
My blood sugar levels have been higher since taking Prednisone. Something to watch out for. But despite that, Couldn't function without Prednisone. It's essential for my inflammatory bowel disease.
Prednisone is a powerful medication, and I'm glad to have it for severe flare-ups. So grateful for Prednisone. It's incredibly effective for severe allergic reactions.
Regular check-ups are crucial when taking Prednisone to monitor for potential issues. I've had some stomach issues and heartburn since starting Prednisone. It's uncomfortable.
Prednisone helped me get through a tough period of chronic pain. It's a powerful medication. However, I get frequent headaches when I'm on Prednisone. It's a persistent issue.
Prednisone has been part of my treatment plan for years. It's a complex drug. This medication is truly effective. It reduced my swelling and pain significantly.
Prednisone has been a lifesaver for my condition. The inflammation went down significantly. However, My appetite increased dramatically with Prednisone, leading to constant cravings.
The fluid retention from Prednisone is noticeable, making me feel bloated. But despite that, My doctor prescribed Prednisone for my asthma, and it's made a huge difference in my breathing.
I struggle with insomnia every time I take Prednisone. It disrupts my sleep pattern.
Prednisone helped me get through a tough period of chronic pain. It's a powerful medication. I've learned to anticipate some of the side effects of Prednisone and manage them.
Prednisone can be tough on the body. I always feel drained and fatigued.
I'm concerned about the long-term effects of Prednisone on my bones. But despite that, I've tried other treatments, but Prednisone is the only one that consistently works for me.
Withdrawal from Prednisone is no joke. It needs to be tapered very carefully.
I've been taking Prednisone for a while now, and it really helps manage my symptoms. Feeling much better. It's important to follow the dosage instructions for Prednisone carefully to minimize side effects.
So grateful for Prednisone. It's incredibly effective for severe allergic reactions.
Withdrawal from Prednisone is no joke. It needs to be tapered very carefully. Prednisone is a powerful medication, and I'm glad to have it for severe flare-ups.
I always make sure to take Prednisone with food to avoid stomach upset. Prednisone gives me anxiety and makes me feel jittery. It's hard to cope with.
I've learned to anticipate some of the side effects of Prednisone and manage them. The 'moon face' side effect from Prednisone is real and affects my self-esteem.
I appreciate the quick action of Prednisone when I need immediate relief.
Couldn't function without Prednisone. It's essential for my inflammatory bowel disease. My doctor explained the pros and cons of Prednisone thoroughly. It's a necessary evil for my condition.
My doctor prescribed Prednisone for my asthma, and it's made a huge difference in my breathing. However, Withdrawal from Prednisone is no joke. It needs to be tapered very carefully.
I appreciate the quick action of Prednisone when I need immediate relief. My blood sugar levels have been higher since taking Prednisone. Something to watch out for.
This medication is truly effective. It reduced my swelling and pain significantly.
The fluid retention from Prednisone is noticeable, making me feel bloated. It's important to follow the dosage instructions for Prednisone carefully to minimize side effects.
I appreciate the quick action of Prednisone when I need immediate relief. I'm impressed with how quickly Prednisone alleviated my severe rash. It's a powerful steroid.
Prednisone works differently for everyone, but for me, the benefits outweigh the drawbacks.
Withdrawal from Prednisone is no joke. It needs to be tapered very carefully. But despite that, This medication is truly effective. It reduced my swelling and pain significantly.
I've learned to anticipate some of the side effects of Prednisone and manage them. Prednisone can be tough on the body. I always feel drained and fatigued.
It's a strong steroid, so I try to use Prednisone only when absolutely necessary. Couldn't function without Prednisone. It's essential for my inflammatory bowel disease.
Regular check-ups are crucial when taking Prednisone to monitor for potential issues.
Prednisone is a short-term solution for me, and it does its job well.
Prednisone worked wonders for my autoimmune disease. I can finally live a more normal life. My experience with Prednisone has been mostly positive, despite some minor side effects.
I've been taking Prednisone for a while now, and it really helps manage my symptoms. Feeling much better. However, Withdrawal from Prednisone is no joke. It needs to be tapered very carefully.
I've noticed my skin becoming thinner and more fragile with long-term Prednisone use. But despite that, Prednisone is a game-changer for acute flare-ups. It provides quick relief.
Prednisone is a strong medication, but it's been very effective in treating my lupus symptoms. I appreciate the quick action of Prednisone when I need immediate relief.
Leave a Review
How Does It Work?
Research
Read our comprehensive review to understand the medication
Consult Your Doctor
Discuss the medication with your healthcare provider
Get Your Prescription
Obtain a valid prescription from your doctor