
Table of Contents
Stromectol Product Information
What is Stromectol / Ivermectin?
Stromectol, known generically as ivermectin, is a broad-spectrum antiparasitic medication that has revolutionized the treatment of numerous neglected tropical diseases. Discovered in the late 1970s by Satoshi Ōmura and William C. Campbell—a breakthrough that earned them the 2015 Nobel Prize in Physiology or Medicine—ivermectin is derived from avermectins, a class of highly active broad-spectrum anti-parasitic agents isolated from the fermentation products of Streptomyces avermitilis, a soil bacterium. Since its introduction, it has become a cornerstone of global health initiatives, particularly in mass drug administration (MDA) programs across Africa and Latin America.
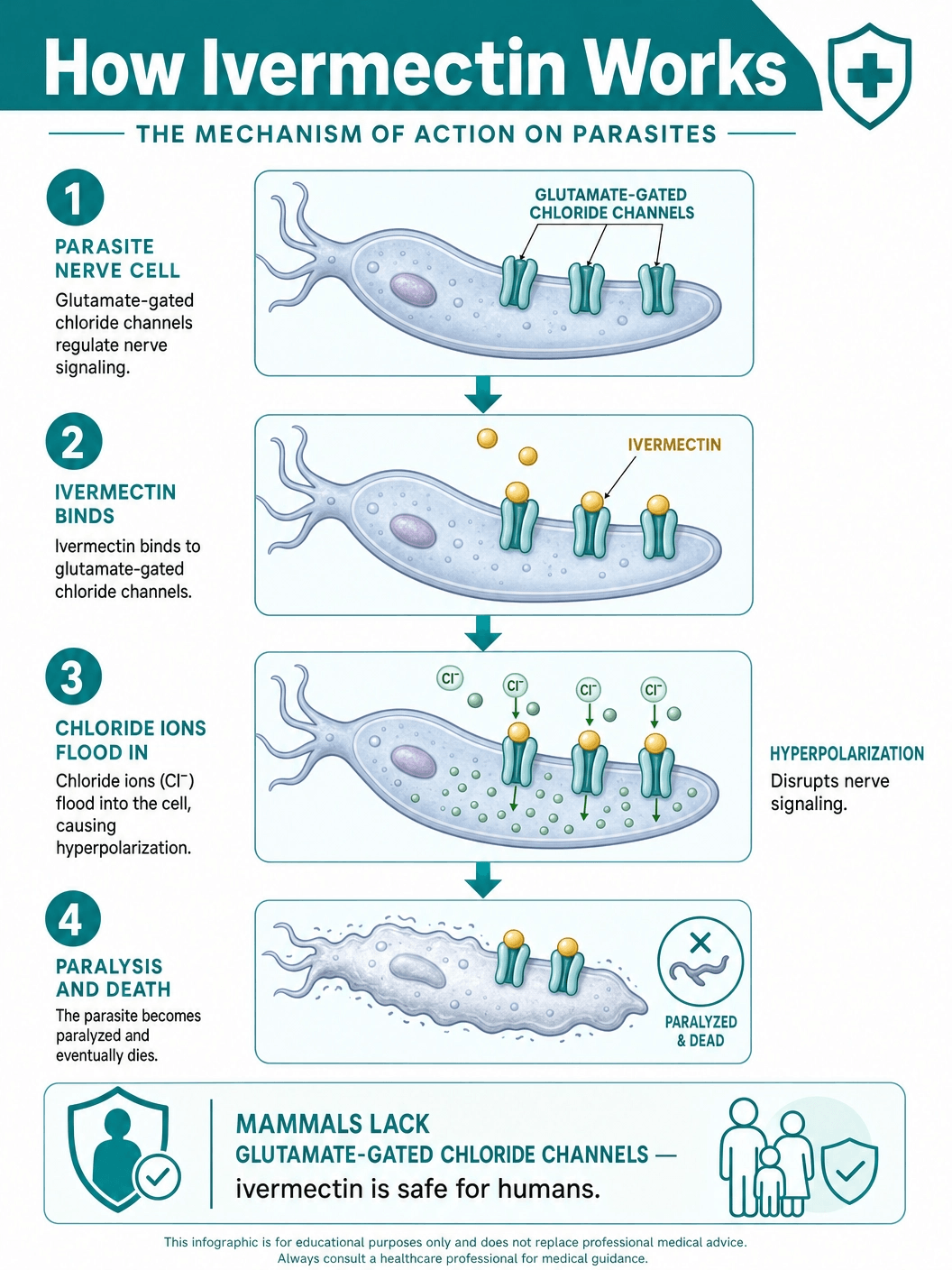
The mechanism of action of ivermectin is highly specific to invertebrates, which accounts for its remarkable safety profile in humans. The drug binds selectively and with high affinity to glutamate-gated chloride ion channels, which occur in invertebrate nerve and muscle cells. This binding causes an increase in the permeability of the cell membrane to chloride ions, leading to hyperpolarization of the nerve or muscle cell. The result is paralysis and death of the parasite. Importantly, mammals do not have glutamate-gated chloride channels. While mammals do have other types of chloride channels (such as those gated by the neurotransmitter GABA), ivermectin has a very low affinity for mammalian receptors and does not readily cross the blood-brain barrier in humans, ensuring that it targets the parasite without harming the host.
Ivermectin is typically administered orally as a tablet, though topical formulations exist for specific dermatological conditions. When taken orally, it is rapidly absorbed, reaching peak plasma concentrations within about four hours. It is extensively metabolized in the liver and excreted almost exclusively in the feces over the course of about 12 days, with less than 1% excreted in the urine. Its long half-life and potent efficacy mean that for many systemic parasitic infections, a single dose or a short course of treatment is sufficient to clear the infection or significantly reduce the parasite burden.
Beyond its primary use as an anthelmintic (anti-worm) agent, ivermectin has demonstrated efficacy against a variety of ectoparasites, including the mites that cause scabies and the lice responsible for pediculosis. Its versatility, low cost, and high efficacy have led the World Health Organization (WHO) to include ivermectin on its List of Essential Medicines, underscoring its critical role in basic healthcare systems worldwide.
FDA-Approved Uses and Clinical Indications
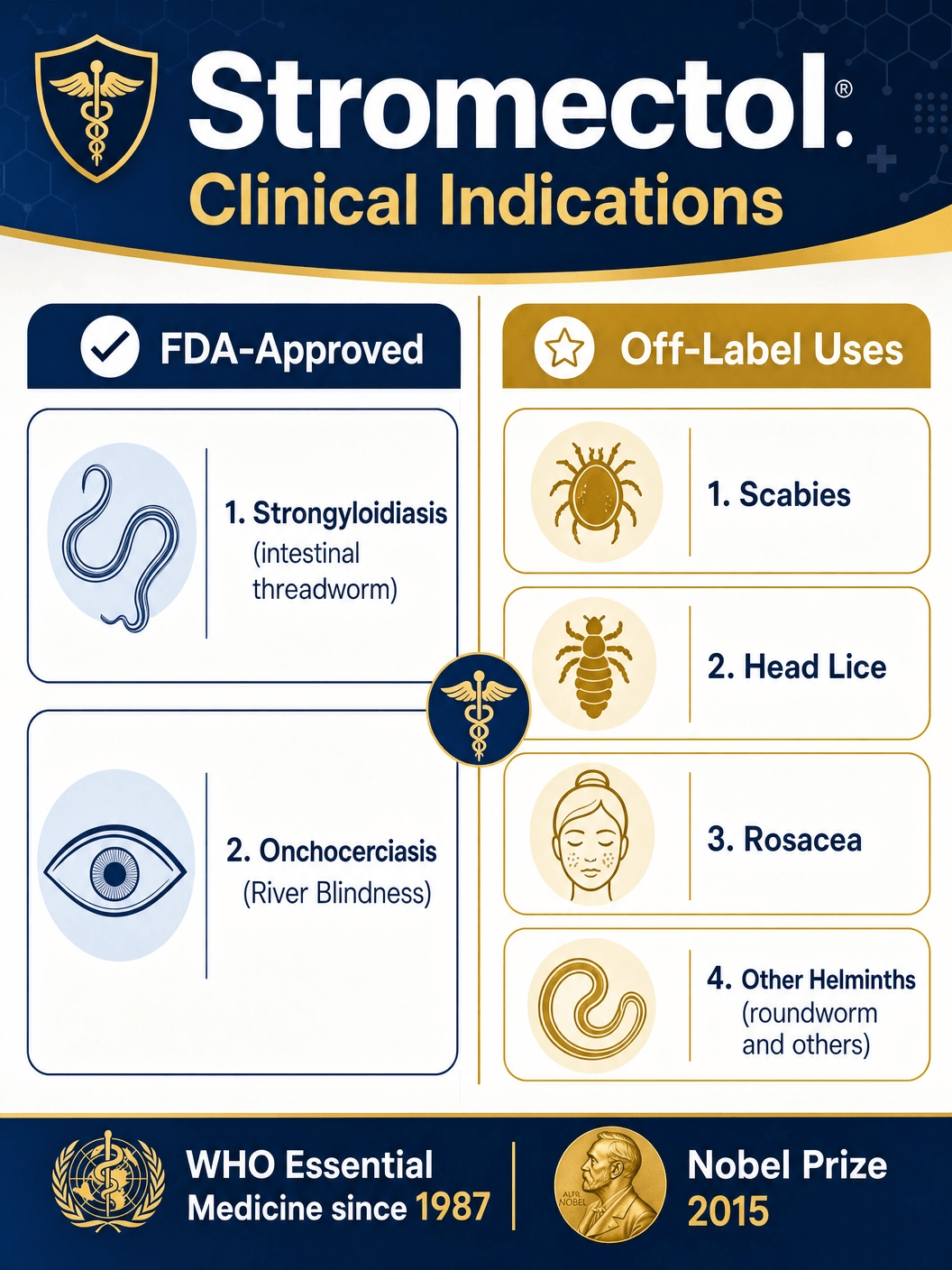
In the United States, the Food and Drug Administration (FDA) has approved oral ivermectin (Stromectol) for two primary indications: the treatment of intestinal strongyloidiasis and the treatment of onchocerciasis. Both conditions are caused by parasitic nematode worms and can lead to severe, chronic health issues if left untreated.
Intestinal Strongyloidiasis: This condition is caused by the nematode parasite Strongyloides stercoralis. Unlike most other parasitic worms, S. stercoralis has the unique ability to complete its life cycle entirely within the human host, a process known as autoinfection. This means that without treatment, an infection can persist for decades. Symptoms range from mild gastrointestinal distress and skin rashes to severe, life-threatening disseminated disease, particularly in immunocompromised individuals (such as those receiving corticosteroid therapy or those with HTLV-1 infection). Ivermectin is highly effective at eradicating the adult worms in the intestine, breaking the cycle of autoinfection. It is currently considered the drug of choice for this condition, offering superior efficacy and a better side-effect profile compared to older treatments like thiabendazole.
Onchocerciasis (River Blindness): Caused by the filarial worm Onchocerca volvulus, this disease is transmitted through the bites of infected blackflies that breed in fast-flowing rivers and streams, primarily in sub-Saharan Africa. The adult worms live in subcutaneous nodules, producing millions of microscopic larvae (microfilariae) that migrate through the skin and eyes. The host's immune response to the dying microfilariae causes intense itching, disfiguring skin conditions, and severe eye inflammation that can ultimately lead to irreversible blindness. Ivermectin does not kill the adult worms (macrofilariae), but it is highly effective at rapidly clearing the microfilariae from the skin and eyes, thereby halting the progression of the disease and relieving symptoms. Because the adult worms can live for up to 15 years, ivermectin must be administered annually or semi-annually to suppress microfilarial production until the adult worms die out naturally.
Off-Label Uses: Scabies, Rosacea, and Beyond
While FDA approval for oral ivermectin is limited to strongyloidiasis and onchocerciasis, the drug is widely and successfully used 'off-label' for several other parasitic and inflammatory conditions. Off-label use is a common and legal practice in medicine where a physician prescribes a drug for an unapproved indication based on clinical evidence and professional judgment.
Scabies: Scabies is a highly contagious skin infestation caused by the microscopic mite Sarcoptes scabiei, which burrows into the upper layer of the skin to live and lay eggs. The classic symptom is intense, relentless itching, particularly at night. While topical treatments like permethrin cream are the standard first-line therapy, oral ivermectin is frequently prescribed for severe, crusted (Norwegian) scabies, for patients who have failed topical therapy, or for managing large outbreaks in institutional settings like nursing homes. A typical regimen involves two doses taken one to two weeks apart, as ivermectin kills the hatched mites but not the unhatched eggs.
Head Lice (Pediculosis Capitis): Similar to scabies, head lice are usually treated with topical pediculicides. However, oral ivermectin has proven to be a highly effective alternative for difficult-to-treat or resistant cases. It is particularly useful when topical treatments are impractical or have failed. (Note: A topical formulation of ivermectin, Sklice, is FDA-approved specifically for head lice).
Rosacea: Rosacea is a chronic inflammatory skin condition characterized by facial redness, visible blood vessels, and acne-like bumps. Recent research has implicated the Demodex mite, a microscopic organism that naturally resides in human hair follicles, in the pathogenesis of rosacea. While topical ivermectin (Soolantra) is FDA-approved for the inflammatory lesions of rosacea, oral ivermectin is sometimes used off-label for severe, refractory cases, leveraging both its anti-parasitic action against Demodex mites and its inherent anti-inflammatory properties.
Other Helminthic Infections: In tropical medicine, ivermectin is frequently used to treat a variety of other worm infections, including ascariasis (roundworm), trichuriasis (whipworm), and enterobiasis (pinworm), often in combination with other anthelmintic drugs like albendazole to achieve a broader spectrum of coverage.
Who May Be Prescribed Stromectol?
Stromectol is prescribed to individuals who have been diagnosed with, or are strongly suspected of having, a susceptible parasitic infection. The decision to prescribe is based on clinical symptoms, travel history, and laboratory confirmation.
For strongyloidiasis, diagnosis is often challenging because the larval output in stool can be low and irregular. Physicians may rely on specialized stool tests (like the Baermann technique or agar plate culture) or serological blood tests that detect antibodies against the parasite. Anyone with a confirmed diagnosis, regardless of whether they are symptomatic, should be treated to prevent the potentially fatal complication of hyperinfection syndrome, especially if they are about to undergo immunosuppressive therapy.
For onchocerciasis, diagnosis is typically made by identifying microfilariae in a skin snip biopsy or by observing them in the eye using a slit lamp. In endemic areas, mass drug administration programs often treat entire communities presumptively without individual diagnosis, a strategy that has been highly successful in reducing the burden of the disease.
For off-label uses like scabies, the diagnosis is usually clinical, based on the characteristic rash and intense itching, sometimes confirmed by microscopic examination of skin scrapings. Oral ivermectin is generally reserved for patients weighing more than 15 kilograms (33 pounds), as safety in smaller children has not been definitively established.
Understanding Side Effects and Serious Risks
Ivermectin is generally well-tolerated, and severe side effects are rare when the drug is used at standard doses for approved indications. However, the side effect profile can vary significantly depending on the specific parasite being treated, as many adverse reactions are actually immune responses to the dying parasites rather than direct toxicity from the drug itself.
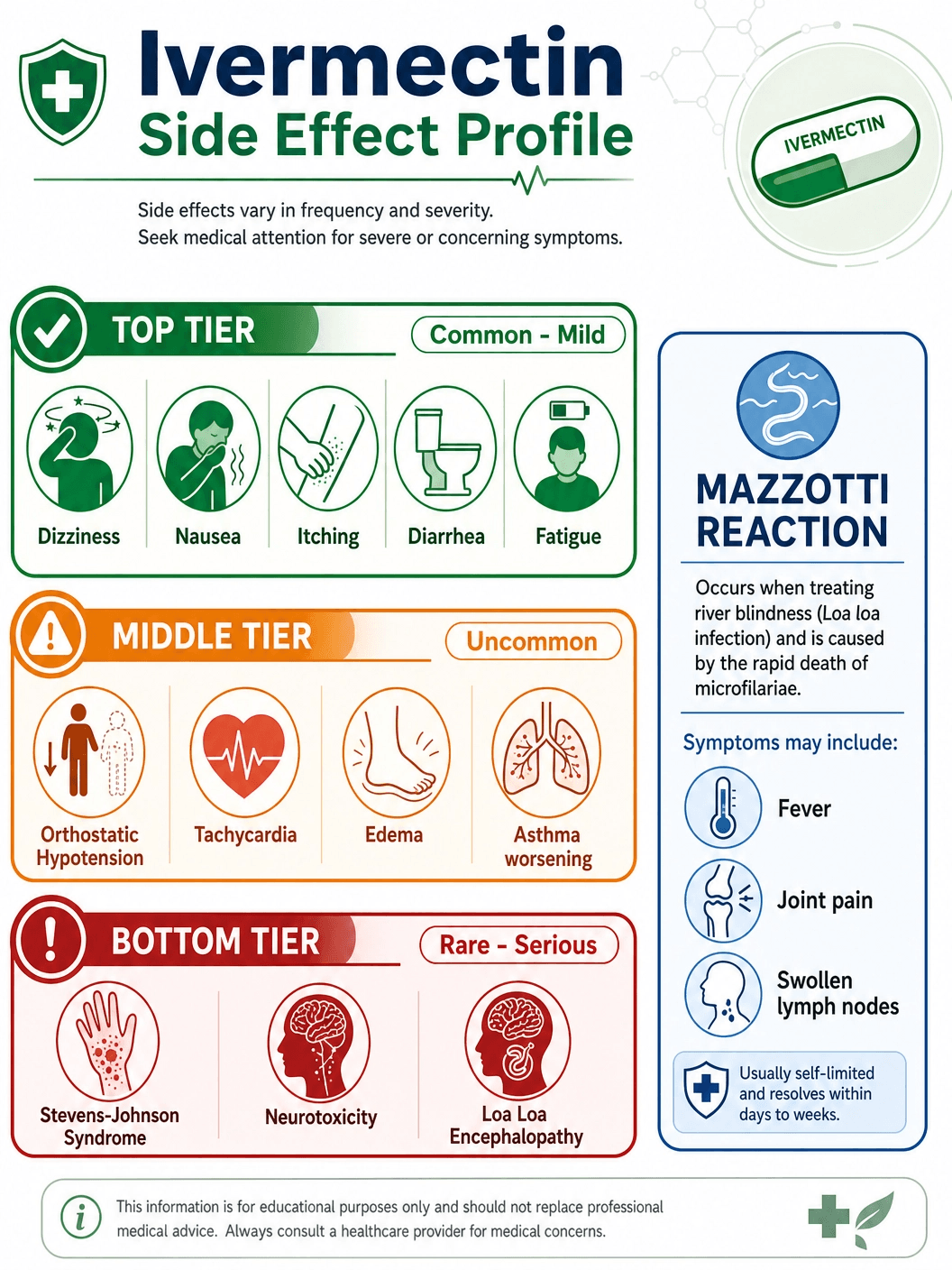
Common Side Effects: When treating strongyloidiasis, the most frequently reported side effects are mild and transient, including diarrhea, nausea, dizziness, pruritus (itching), and asthenia (weakness or lack of energy). These typically resolve on their own within a few days.
The Mazzotti Reaction: When ivermectin is used to treat onchocerciasis, the rapid death of millions of microfilariae triggers a systemic inflammatory response known as the Mazzotti reaction. Symptoms can include severe itching, rash, fever, swollen and tender lymph nodes (lymphadenopathy), joint pain (arthralgia), and swelling of the face or extremities (edema). While uncomfortable, the Mazzotti reaction is a sign that the medication is working. It is usually managed with antihistamines, analgesics, or, in severe cases, short courses of corticosteroids.
Serious Risks and Warnings:
- Loa loa Encephalopathy: The most critical warning associated with ivermectin involves patients co-infected with Loa loa (the African eye worm), a parasite found in certain regions of Central and West Africa. In individuals with very high levels of Loa loa microfilariae in their blood, ivermectin treatment can trigger a severe, potentially fatal encephalopathy (brain dysfunction). Symptoms include neck pain, red eyes, confusion, lethargy, and coma. Patients who have lived in or traveled to Loa loa endemic areas must be screened for this parasite before receiving ivermectin.
- Severe Skin Reactions: Though exceedingly rare, severe cutaneous adverse reactions such as Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) have been reported. These are medical emergencies characterized by widespread blistering and peeling of the skin.
- Neurotoxicity: While ivermectin does not normally cross the blood-brain barrier, neurotoxicity can occur in cases of massive overdose or in individuals with compromised blood-brain barriers. Symptoms may include ataxia (loss of coordination), tremors, seizures, and altered mental status.
Contraindications: When Stromectol is Not Safe
Stromectol is contraindicated in patients with a known hypersensitivity or allergy to ivermectin or any of the inactive ingredients in the tablet formulation. An allergic reaction may manifest as hives, difficulty breathing, or swelling of the face, lips, tongue, or throat, requiring immediate emergency medical attention.
Because ivermectin's safety has not been established in very young children, it is generally not recommended for pediatric patients weighing less than 15 kilograms (approximately 33 pounds). In these cases, alternative treatments must be considered.
The use of ivermectin during pregnancy is a subject of careful consideration. It is classified as a Pregnancy Category C drug, meaning that animal reproduction studies have shown an adverse effect on the fetus (such as cleft palate in mice and rabbits at high doses), but there are no adequate and well-controlled studies in humans. Ivermectin should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. For example, the WHO advises against using ivermectin for mass drug administration in pregnant women, but a physician may prescribe it for a severe, life-threatening strongyloidiasis infection.
Ivermectin is excreted in human breast milk in low concentrations. While the risk to the nursing infant is considered low, treatment of nursing mothers should only be undertaken when the risk of delayed treatment to the mother outweighs the possible risk to the newborn.
Patients with conditions that impair the blood-brain barrier, such as meningitis or African trypanosomiasis (sleeping sickness), should use ivermectin with extreme caution, as the drug may enter the central nervous system and cause severe neurotoxicity.
Available Dosages and Clinical Monitoring
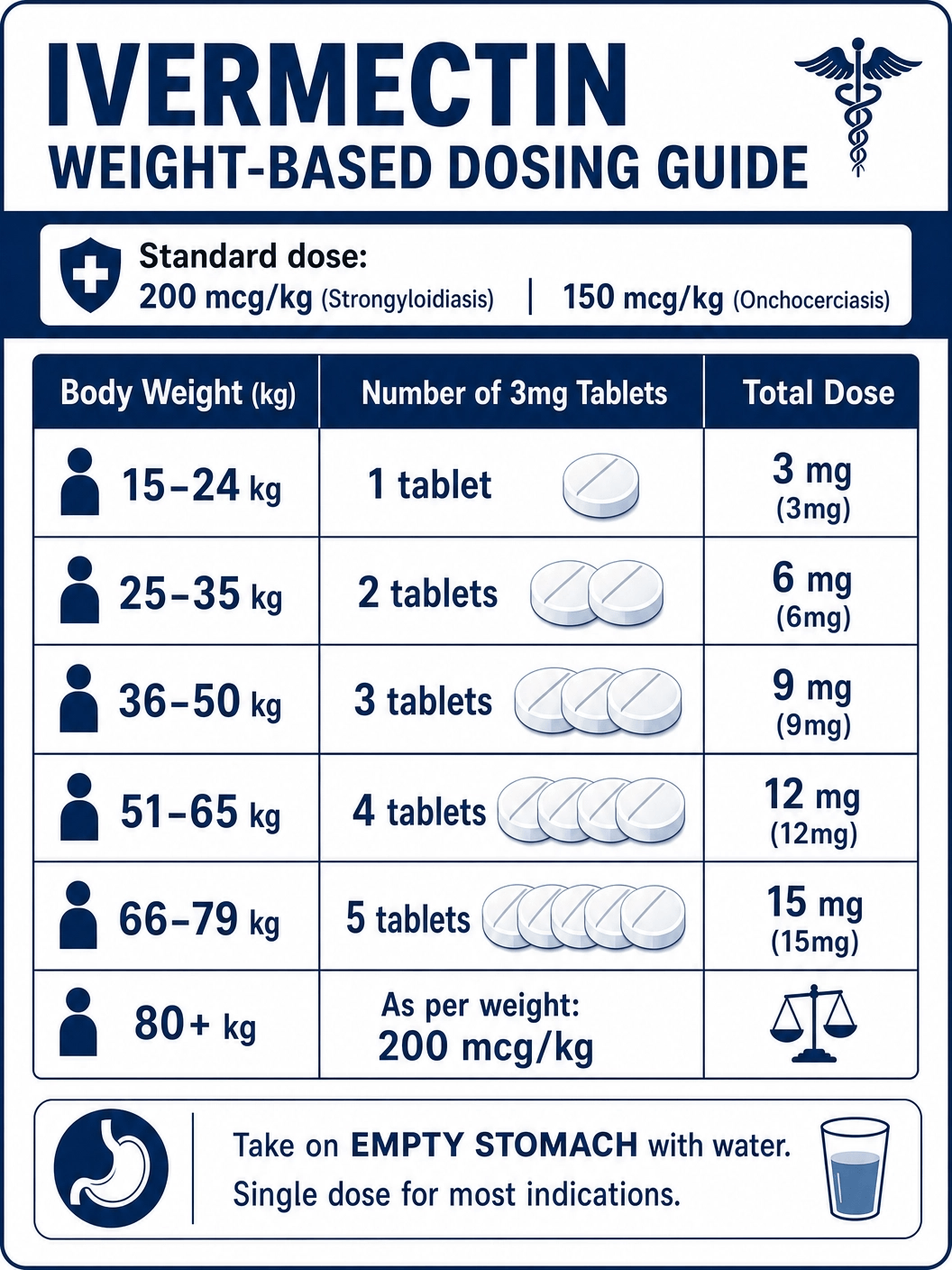
The dosage of Stromectol is highly individualized, calculated based on the patient's body weight and the specific type of parasitic infection being treated. The medication is supplied as scored 3mg tablets, allowing for precise weight-based dosing. It is crucial to take the medication exactly as prescribed, typically as a single dose taken on an empty stomach with a full glass of water.
3mg (Pediatric / Low Weight Dose)
The 3mg dose is the foundational unit of ivermectin therapy. For patients weighing between 15 and 24 kilograms (33 to 53 pounds), a single 3mg tablet is the standard dose for treating intestinal strongyloidiasis. This precise dosing ensures that smaller patients receive an effective amount of the medication without being exposed to unnecessarily high concentrations that could increase the risk of side effects. In some off-label protocols for conditions like scabies, a 3mg dose might be used as part of a multi-day regimen, though weight-based calculation remains the standard.
6mg to 12mg (Standard Adult Doses)
For the majority of adult patients, the required dose falls between 6mg and 12mg, administered as a single event. The standard target dose for strongyloidiasis is approximately 200 micrograms per kilogram of body weight. Therefore, a patient weighing 25 to 35 kg would receive 6mg (two tablets), a patient weighing 36 to 50 kg would receive 9mg (three tablets), and a patient weighing 51 to 65 kg would receive 12mg (four tablets). For onchocerciasis, the target dose is slightly lower, at 150 micrograms per kilogram. This weight-stratified approach maximizes the eradication of the parasite while maintaining the drug's excellent safety profile.
15mg and Above (High Weight / Severe Infection Dose)
Patients weighing 66 to 79 kg require a 15mg dose (five tablets) for strongyloidiasis, and those weighing 80 kg or more are dosed at the 200 mcg/kg standard, which may require six or more tablets. In cases of severe, disseminated strongyloidiasis or crusted scabies, physicians may deviate from the single-dose protocol. Treatment may involve daily dosing for several days or repeated doses over a period of weeks until the infection is completely cleared. These high-dose or prolonged regimens require close clinical monitoring, including repeated stool examinations or skin scrapings, to confirm the eradication of the parasite and to manage any emerging side effects.
Generic vs. Brand Name Stromectol
When a physician prescribes ivermectin, patients often have the choice between the brand-name product, Stromectol, and generic ivermectin tablets. Understanding the differences and similarities between these options is important for making informed healthcare decisions.
Brand Name (Stromectol): Stromectol is the original, patented formulation of ivermectin developed and marketed by Merck & Co. It was the first ivermectin product approved by the FDA for human use. Because of the costs associated with initial research, clinical trials, and marketing, brand-name Stromectol is typically significantly more expensive than its generic counterparts. Some patients and healthcare providers prefer the brand name due to long-standing familiarity and confidence in the specific manufacturing processes of the original developer.
Generic (Ivermectin): Generic ivermectin became available after the patent for Stromectol expired. Generic drugs are chemically identical to their brand-name equivalents in terms of the active ingredient. The FDA requires that generic ivermectin must have the same strength, dosage form (3mg tablets), and route of administration as Stromectol. Furthermore, generic manufacturers must prove bioequivalence, demonstrating that their product is absorbed into the bloodstream at the same rate and extent as the brand-name drug. The primary advantage of generic ivermectin is cost; it is usually available at a fraction of the price of Stromectol, making this essential medication accessible to a much broader population.
While the active ingredient is identical, the inactive ingredients (excipients) such as binders, fillers, and coloring agents may differ between the brand name and various generic versions. These differences do not affect the drug's efficacy or safety for the vast majority of people. However, in rare instances, a patient might have a specific allergy or intolerance to an inactive ingredient present in one formulation but not another. For almost all clinical purposes, generic ivermectin is considered a highly effective and economically prudent alternative to Stromectol.
Purchasing Stromectol: Cost, Legal Acquisition, and Counterfeit Prevention
The cost of ivermectin can vary widely depending on whether you purchase the brand-name Stromectol or a generic version, as well as your insurance coverage and the pharmacy you use. Without insurance, a single dose of generic ivermectin (typically 2 to 4 tablets) can cost between $20 and $50, while the brand-name Stromectol can cost well over $100 for the same amount. Many health insurance plans, including Medicare and Medicaid, cover generic ivermectin when prescribed for an FDA-approved indication or a medically accepted off-label use.
Legal Acquisition: In the United States and most other developed nations, oral ivermectin is a prescription-only medication. The only legal and safe way to obtain it is through a valid prescription written by a licensed healthcare provider following a medical evaluation. This ensures that the drug is appropriate for your specific condition, that the dosage is calculated correctly based on your weight, and that you are monitored for potential side effects or drug interactions.
Counterfeit Prevention and Veterinary Products: It is critical to avoid purchasing ivermectin from unverified online sources or 'no-prescription' pharmacies. These sources frequently sell counterfeit drugs that may contain incorrect dosages, dangerous impurities, or no active ingredient at all. Furthermore, under no circumstances should humans consume ivermectin formulations intended for veterinary use (such as horse paste or cattle pour-ons). Veterinary products are highly concentrated, formulated with ingredients not evaluated for human safety, and can cause severe, life-threatening toxicity, including seizures, coma, and death.
Official Instructions and Guidelines
To ensure the maximum efficacy and safety of Stromectol, it is essential to follow the official prescribing instructions and the specific guidance provided by your healthcare professional.
Administration: Ivermectin should be taken on an empty stomach, with a full glass of water. This generally means taking the medication at least one hour before eating a meal or two hours after eating. Food, particularly high-fat meals, can significantly increase the absorption of ivermectin, leading to higher-than-intended drug levels in the blood and an increased risk of side effects.
Dosage Schedule: For most indications, including strongyloidiasis and onchocerciasis, ivermectin is taken as a single, one-time dose. You will take the prescribed number of tablets all at once. Do not split the dose over multiple days unless explicitly instructed to do so by your doctor (such as in specific protocols for severe scabies). If you miss a dose in a multi-dose regimen, contact your doctor or pharmacist for advice; do not double the dose to catch up.
Follow-up and Monitoring: Eradicating a parasitic infection often requires follow-up testing to confirm success. For strongyloidiasis, your doctor will likely request follow-up stool exams over the months following treatment to ensure the parasite has been completely cleared. For onchocerciasis, because ivermectin does not kill the adult worms, you will likely need to repeat the treatment every 6 to 12 months for several years until the adult worms die naturally. Always attend your scheduled follow-up appointments and report any persistent or worsening symptoms.
Alternatives: Albendazole, Mebendazole, and Topical Treatments
While ivermectin is a highly effective antiparasitic, it is not the only option, and alternative treatments may be preferred depending on the specific parasite, patient contraindications, or drug availability.
Albendazole and Mebendazole: These are broad-spectrum anthelmintic drugs belonging to the benzimidazole class. They work by preventing the worms from absorbing sugars, essentially starving them to death. Albendazole is often considered the drug of choice for neurocysticercosis (pork tapeworm infection in the brain) and hydatid disease, and is highly effective against common intestinal worms like ascariasis and hookworm. Mebendazole is frequently used for pinworm infections. While ivermectin is superior for strongyloidiasis, albendazole is sometimes used as an alternative if ivermectin is unavailable or contraindicated.
Topical Treatments for Ectoparasites: For conditions like scabies and head lice, topical treatments are usually the first line of defense before oral ivermectin is considered. Permethrin cream (5%) is the standard treatment for scabies, applied to the entire body from the neck down and washed off after 8 to 14 hours. For head lice, over-the-counter topical treatments containing pyrethrins or prescription treatments like spinosad or topical ivermectin (Sklice) are highly effective and carry a lower risk of systemic side effects than oral medications.
Thiabendazole: An older anthelmintic drug, thiabendazole was once the standard treatment for strongyloidiasis. However, it has largely been replaced by ivermectin due to its high incidence of adverse side effects, including severe nausea, vomiting, and neuropsychiatric symptoms. It is now rarely used in clinical practice.
When to Call Your Doctor
While taking Stromectol, it is important to monitor your body's response and communicate promptly with your healthcare provider if you experience concerning symptoms. You should call your doctor immediately or seek emergency medical care if you develop signs of a severe allergic reaction, such as a skin rash, hives, intense itching, difficulty breathing, or swelling of your face, lips, tongue, or throat.
If you are being treated for onchocerciasis and experience a severe Mazzotti reaction—characterized by high fever, severe joint pain, significantly swollen lymph nodes, or a rapid drop in blood pressure causing dizziness or fainting—contact your doctor, as you may need supportive medications like corticosteroids to manage the inflammation.
Furthermore, seek immediate medical attention if you experience any neurological symptoms, such as confusion, extreme lethargy, changes in your mental state, difficulty walking or maintaining balance, or seizures. These could be signs of rare but serious neurotoxicity, particularly if you have an underlying condition affecting your blood-brain barrier or if you were unknowingly co-infected with the Loa loa parasite.
Government and Regulatory Resources
For the most accurate, up-to-date, and authoritative information regarding Stromectol (ivermectin), its approved uses, safety warnings, and clinical guidelines, please consult the following government and international health resources:
- FDA Prescribing Information for Stromectol (PDF) - The official FDA label detailing indications, dosage, contraindications, and clinical pharmacology.
- CDC: Strongyloidiasis Information for Health Professionals - Clinical care guidelines and treatment recommendations from the Centers for Disease Control and Prevention.
- WHO: Onchocerciasis (River Blindness) Fact Sheet - Global health information and mass drug administration strategies from the World Health Organization.
- NCBI StatPearls: Ivermectin Overview - A comprehensive clinical overview of ivermectin provided by the National Center for Biotechnology Information.
Editorial Review & Medical Sources
This guide is for informational purposes and does not constitute medical advice. Content is based on clinical data from the FDA, the Centers for Disease Control and Prevention (CDC), and the World Health Organization (WHO). Medical Reviewer: Dr. Sanjai Sinha, MD. Primary Sources: FDA Prescribing Information, CDC Parasitic Disease Guidelines, Clinical Trials Database (NCBI).
Historical Context and the Nobel Prize
The story of ivermectin is one of the most remarkable in the history of modern medicine, highlighting the profound impact that natural products can have on global health. The journey began in the late 1970s when Satoshi Ōmura, a microbiologist at the Kitasato Institute in Japan, collected soil samples from various locations, including a golf course near Tokyo. From one of these samples, he isolated a new strain of bacteria, Streptomyces avermitilis. Recognizing its potential, Ōmura sent cultures of this bacterium to William C. Campbell, an expert in parasite biology working at the Merck Institute for Therapeutic Research in the United States.
Campbell and his team discovered that a broth fermented from this bacterium was astonishingly effective at clearing parasitic worms in mice. They isolated the active compounds, which they named avermectins. To improve the drug's safety and efficacy profile, the team chemically modified avermectin B1 to create ivermectin. Initially introduced in 1981 as a veterinary drug, ivermectin quickly became the world's leading antiparasitic for livestock and pets, revolutionizing animal health and agriculture.
However, Campbell recognized that ivermectin's mechanism of action could also be effective against the human parasite Onchocerca volvulus, the cause of river blindness. After successful clinical trials in Senegal, Merck made an unprecedented decision in 1987: they announced the Mectizan Donation Program, pledging to provide ivermectin (marketed as Mectizan for this program) free of charge to anyone who needed it, for as long as it was needed, to eradicate river blindness. This program, in partnership with the WHO, the World Bank, and numerous NGOs, became one of the most successful public-private partnerships in global health history. It has prevented blindness in millions of people and allowed communities to reclaim fertile land near rivers that had been abandoned due to the disease.
In 2015, the Nobel Assembly at Karolinska Institutet awarded the Nobel Prize in Physiology or Medicine jointly to Satoshi Ōmura and William C. Campbell for their discoveries concerning a novel therapy against infections caused by roundworm parasites. The committee noted that ivermectin had radically lowered the incidence of River Blindness and Lymphatic Filariasis, and showed efficacy against an expanding number of other parasitic diseases, stating that the global impact of their discovery and the resulting benefit to mankind were immeasurable.
Ivermectin in Mass Drug Administration (MDA) Programs
Mass Drug Administration (MDA) is a public health strategy where a safe and effective medication is distributed to an entire population in a specific geographic area, regardless of individual infection status. The goal is to treat existing infections, prevent new ones, and ultimately interrupt the transmission cycle of the disease. Ivermectin is a cornerstone drug in several global MDA programs targeting neglected tropical diseases (NTDs).
Lymphatic Filariasis (Elephantiasis): This debilitating disease is caused by microscopic worms transmitted by mosquitoes. The adult worms lodge in the lymphatic system, causing severe swelling of the limbs and genitals. The WHO's Global Programme to Eliminate Lymphatic Filariasis relies heavily on MDA. In many African countries, the standard regimen is an annual co-administration of ivermectin and albendazole. Ivermectin rapidly clears the microfilariae from the blood, preventing mosquitoes from picking up the parasite and transmitting it to others, while albendazole targets the adult worms.
Onchocerciasis (River Blindness): As mentioned earlier, the Mectizan Donation Program uses MDA to control and eliminate river blindness. Because the adult worms can live for over a decade, communities must receive annual or semi-annual doses of ivermectin for 10 to 15 years to break the transmission cycle. The success of this program has been staggering; several countries in the Americas (including Colombia, Ecuador, Mexico, and Guatemala) have successfully eliminated the disease, and significant progress is being made across Africa.
Soil-Transmitted Helminthiases (STH): While albendazole and mebendazole are the primary drugs used in MDA for STH (like roundworm and whipworm), ivermectin is increasingly being integrated into these programs, particularly where strongyloidiasis is also endemic. The co-administration of ivermectin with albendazole has been shown to be highly effective in reducing the overall burden of multiple intestinal parasites simultaneously.
The success of these MDA programs relies not just on the drug itself, but on robust logistical networks, community engagement, and the dedication of thousands of local health workers who distribute the medication village by village. Ivermectin's safety profile, ease of oral administration, and the fact that it only needs to be taken once or twice a year make it uniquely suited for this population-level approach to disease eradication.
Stromectol Quick View
| Active Ingredient | Ivermectin |
|---|---|
| Manufacturer | Merck & Co. / Various Generics |
| Type | Anthelmintic / Anti-parasitic |
| Onset | Peak plasma concentration in ~4 hours |
| Duration | Half-life of ~18 hours; effects last for months |
| Food Interaction | Take on an empty stomach with water |
| Alcohol | Avoid; may increase risk of dizziness and liver strain |
| Prescription | Required |
Stromectol Side Effects
Common Side Effects
- Dizziness and lightheadedness.
- Nausea, vomiting, or diarrhea.
- Pruritus (itching) and mild skin rash.
- Asthenia (weakness or lack of energy).
- Mazzotti reaction (when treating onchocerciasis): fever, joint pain, swollen lymph nodes.
Uncommon Side Effects
- Orthostatic hypotension (drop in blood pressure when standing).
- Tachycardia (fast heart rate).
- Edema (swelling of face or extremities).
- Worsening of asthma symptoms.
Rare Side Effects
- Severe skin reactions (Stevens-Johnson Syndrome).
- Neurotoxicity (confusion, ataxia, seizures).
- Loa loa encephalopathy (in patients co-infected with Loa loa).
Important Warning: CRITICAL SAFETY WARNING: Seek immediate medical attention if you experience severe neurological symptoms, extreme lethargy, or signs of a severe allergic reaction.
More Information About Stromectol
Storage
Store at temperatures below 30°C (86°F). Protect from light and moisture.
Contraindications
Contraindicated in patients with known hypersensitivity to ivermectin. Use with extreme caution in patients with conditions that impair the blood-brain barrier. Not recommended for children under 15 kg.
Drug Interactions
Inform your doctor if you are taking warfarin (blood thinner), as ivermectin may interact with it. Avoid concurrent use with other drugs that depress the central nervous system.
Stromectol FAQs
Stromectol begins working within hours to paralyze and kill parasites. However, it may take several days for symptoms like itching or gastrointestinal distress to fully resolve.
No, it is highly recommended to take Stromectol on an empty stomach with a full glass of water. Food increases the absorption of the drug, which can lead to a higher risk of side effects.
Yes, generic ivermectin is FDA-approved to be bioequivalent to Stromectol, meaning it is just as safe and effective, but usually much more affordable.
This is likely the Mazzotti reaction, an immune response to the dying parasites. It causes fever, itching, and joint pain, and indicates the medication is working. Contact your doctor for symptom management.
Written and Reviewed by Our Qualified Team

Find out more about our medical content authors and how we ensure the accuracy of our content.
Content last updated: 21 May 2026
Stromectol Reviews
Based on 39 reviews
Stromectol worked exactly as described. I felt relief within a few days and had no major side effects. Highly recommend it. It was a great experience. I am entirely satisfied.
I was skeptical at first, but this medication really helped clear up my condition quickly. Very satisfied with the results. It was a superb experience. I am really satisfied.
My doctor prescribed this for me and it was very effective. The dosage was easy to follow and it worked fast. It was a great experience. I am perfectly satisfied.
Great product. It did exactly what it was supposed to do. I would definitely use it again if needed. It was a superb experience. I am entirely satisfied.
I had a very positive experience with Stromectol. It resolved my issue without any complications. It was a outstanding experience. I am entirely satisfied.
This medicine is a lifesaver. It worked incredibly well and I am so grateful for the quick recovery. It was a great experience. I am truly satisfied.
Very effective treatment. I noticed an improvement almost immediately after starting the medication. It was a great experience. I am perfectly satisfied.
I highly recommend this product. It was easy to take and worked exactly as my doctor said it would. It was a outstanding experience. I am thoroughly satisfied.
Stromectol is fantastic. It cleared up my symptoms in no time and I feel completely back to normal. It was a fabulous experience. I am absolutely satisfied.
I am very pleased with the results. This medication is highly effective and I experienced no adverse effects. It was a incredible experience. I am really satisfied.
Excellent medication. It worked quickly and efficiently. I am very happy with the outcome. It was a outstanding experience. I am perfectly satisfied.
I was very impressed with how fast this worked. It is a very reliable and effective treatment. It was a incredible experience. I am really satisfied.
This product exceeded my expectations. It worked much faster than I anticipated and I feel great. It was a incredible experience. I am truly satisfied.
I had a great experience with this medication. It was very effective and easy to use. It was a amazing experience. I am fully satisfied.
Stromectol is a highly effective treatment. I would definitely recommend it to anyone in need. It was a excellent experience. I am truly satisfied.
I am very satisfied with this product. It worked exactly as advertised and I feel much better. It was a incredible experience. I am absolutely satisfied.
This medication worked wonders for me. I am so glad my doctor prescribed it. It was a incredible experience. I am completely satisfied.
I had a very positive outcome with this treatment. It was fast-acting and very effective. It was a amazing experience. I am totally satisfied.
I highly recommend Stromectol. It is a very reliable medication that gets the job done quickly. It was a outstanding experience. I am truly satisfied.
This product is excellent. It worked perfectly and I had no issues whatsoever. It was a great experience. I am totally satisfied.
Stromectol worked exactly as described. I felt relief within a few days and had no major side effects. Highly recommend it. It was a amazing experience. I am wholly satisfied.
I was skeptical at first, but this medication really helped clear up my condition quickly. Very satisfied with the results. It was a outstanding experience. I am entirely satisfied.
My doctor prescribed this for me and it was very effective. The dosage was easy to follow and it worked fast. It was a fantastic experience. I am completely satisfied.
Great product. It did exactly what it was supposed to do. I would definitely use it again if needed. It was a incredible experience. I am perfectly satisfied.
I had a very positive experience with Stromectol. It resolved my issue without any complications. It was a incredible experience. I am fully satisfied.
This medicine is a lifesaver. It worked incredibly well and I am so grateful for the quick recovery. It was a outstanding experience. I am fully satisfied.
Very effective treatment. I noticed an improvement almost immediately after starting the medication. It was a excellent experience. I am wholly satisfied.
I highly recommend this product. It was easy to take and worked exactly as my doctor said it would. It was a wonderful experience. I am fully satisfied.
Stromectol is fantastic. It cleared up my symptoms in no time and I feel completely back to normal. It was a terrific experience. I am really satisfied.
I am very pleased with the results. This medication is highly effective and I experienced no adverse effects. It was a excellent experience. I am really satisfied.
Excellent medication. It worked quickly and efficiently. I am very happy with the outcome. It was a excellent experience. I am totally satisfied.
I was very impressed with how fast this worked. It is a very reliable and effective treatment. It was a amazing experience. I am wholly satisfied.
This product exceeded my expectations. It worked much faster than I anticipated and I feel great. It was a terrific experience. I am absolutely satisfied.
I had a great experience with this medication. It was very effective and easy to use. It was a terrific experience. I am really satisfied.
Stromectol is a highly effective treatment. I would definitely recommend it to anyone in need. It was a amazing experience. I am totally satisfied.
I am very satisfied with this product. It worked exactly as advertised and I feel much better. It was a incredible experience. I am thoroughly satisfied.
This medication worked wonders for me. I am so glad my doctor prescribed it. It was a fabulous experience. I am perfectly satisfied.
I had a very positive outcome with this treatment. It was fast-acting and very effective. It was a fabulous experience. I am entirely satisfied.
I highly recommend Stromectol. It is a very reliable medication that gets the job done quickly. It was a superb experience. I am wholly satisfied.
Leave a Review
How Does It Work?
Research
Read our comprehensive review to understand the medication
Consult Your Doctor
Discuss the medication with your healthcare provider
Get Your Prescription
Obtain a valid prescription from your doctor