
Synthroid (AbbVie)
General Health Treatment
Synthroid (Levothyroxine) is a synthetic thyroid hormone used to treat hypothyroidism and manage well-differentiated thyroid cancer.
Table of Contents
Synthroid Product Information
What is Synthroid (Levothyroxine)?
Synthroid, known generically as levothyroxine sodium, is a synthetic version of thyroxine (T4), the primary hormone produced by the human thyroid gland. It is one of the most widely prescribed medications in the world, serving as the cornerstone of treatment for hypothyroidism—a condition where the thyroid gland fails to produce enough hormones to meet the body's metabolic needs.
The thyroid gland, a small butterfly-shaped organ located at the base of the neck, acts as the body's master metabolic control center. The hormones it produces dictate how fast the body uses energy, consumes oxygen, and produces heat. When the thyroid is underactive, every system in the body slows down. Synthroid is designed to perfectly mimic the body's natural T4, restoring normal metabolic function and alleviating the debilitating symptoms of hypothyroidism.
Mechanism of Action: How Levothyroxine Works
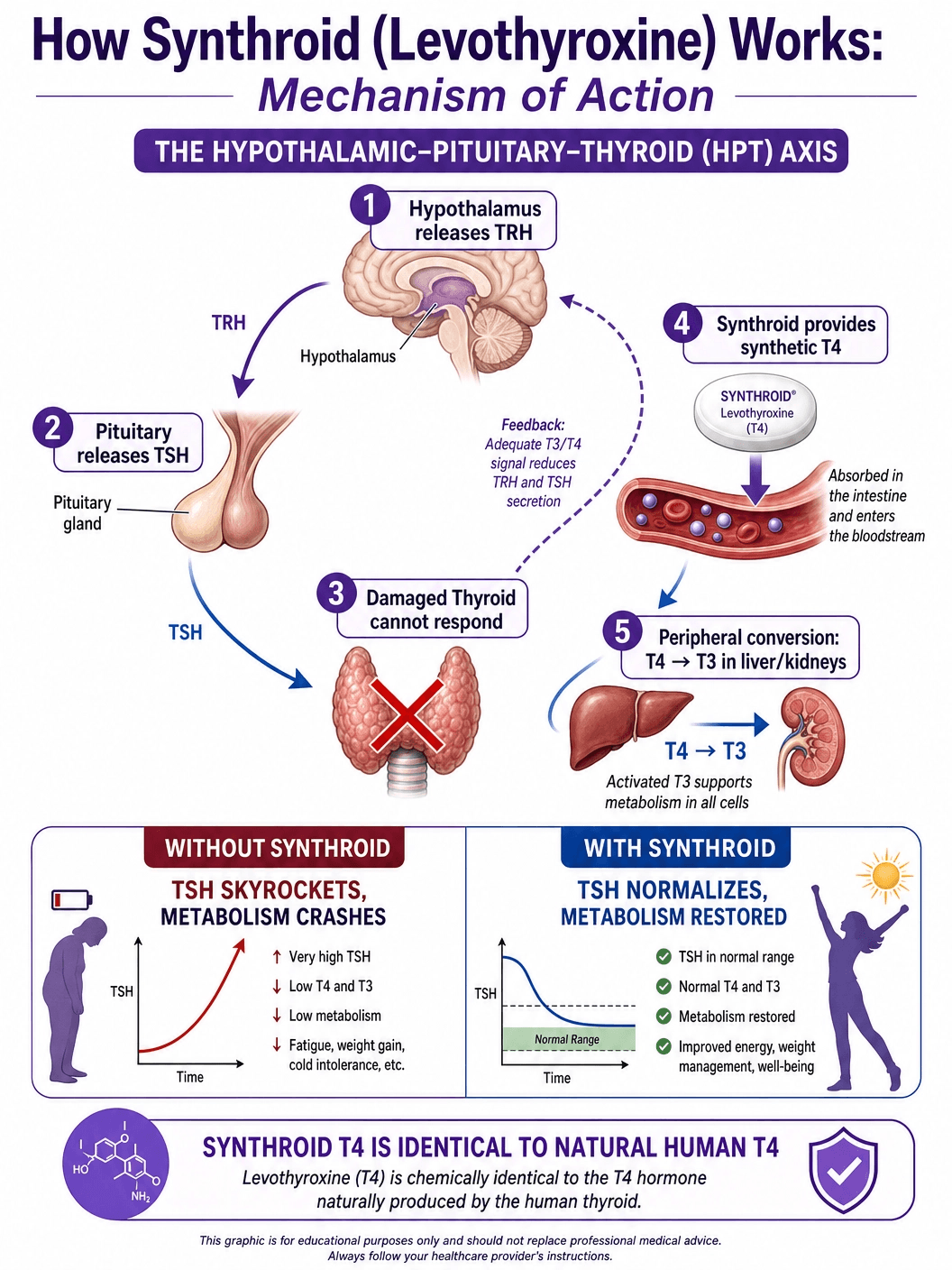
To understand how Synthroid works, one must first understand the hypothalamic-pituitary-thyroid (HPT) axis, the complex feedback loop that regulates thyroid function.
The Natural Feedback Loop: The hypothalamus in the brain releases Thyrotropin-Releasing Hormone (TRH), which signals the pituitary gland to release Thyroid-Stimulating Hormone (TSH). TSH then travels to the thyroid gland, stimulating it to produce and release two main hormones: thyroxine (T4) and triiodothyronine (T3). T4 is the inactive "storage" form, while T3 is the active form that cells actually use. The body constantly monitors the levels of T4 and T3 in the blood; if they drop too low, the pituitary releases more TSH to stimulate production. If they are too high, TSH production is suppressed.
The Role of Synthroid: In primary hypothyroidism (most commonly caused by Hashimoto's thyroiditis, an autoimmune disease), the thyroid gland is damaged and cannot respond to TSH. As a result, T4 and T3 levels plummet, and TSH levels skyrocket as the pituitary desperately tries to stimulate the failing gland. Synthroid provides a steady, exogenous supply of synthetic T4. Once absorbed into the bloodstream, this synthetic T4 is indistinguishable from natural T4. The body's peripheral tissues (like the liver and kidneys) then convert this T4 into the active T3 hormone exactly as they would with naturally produced T4. This restores normal metabolic rates and signals the pituitary gland to lower its TSH production back to a normal range.
FDA-Approved Indications
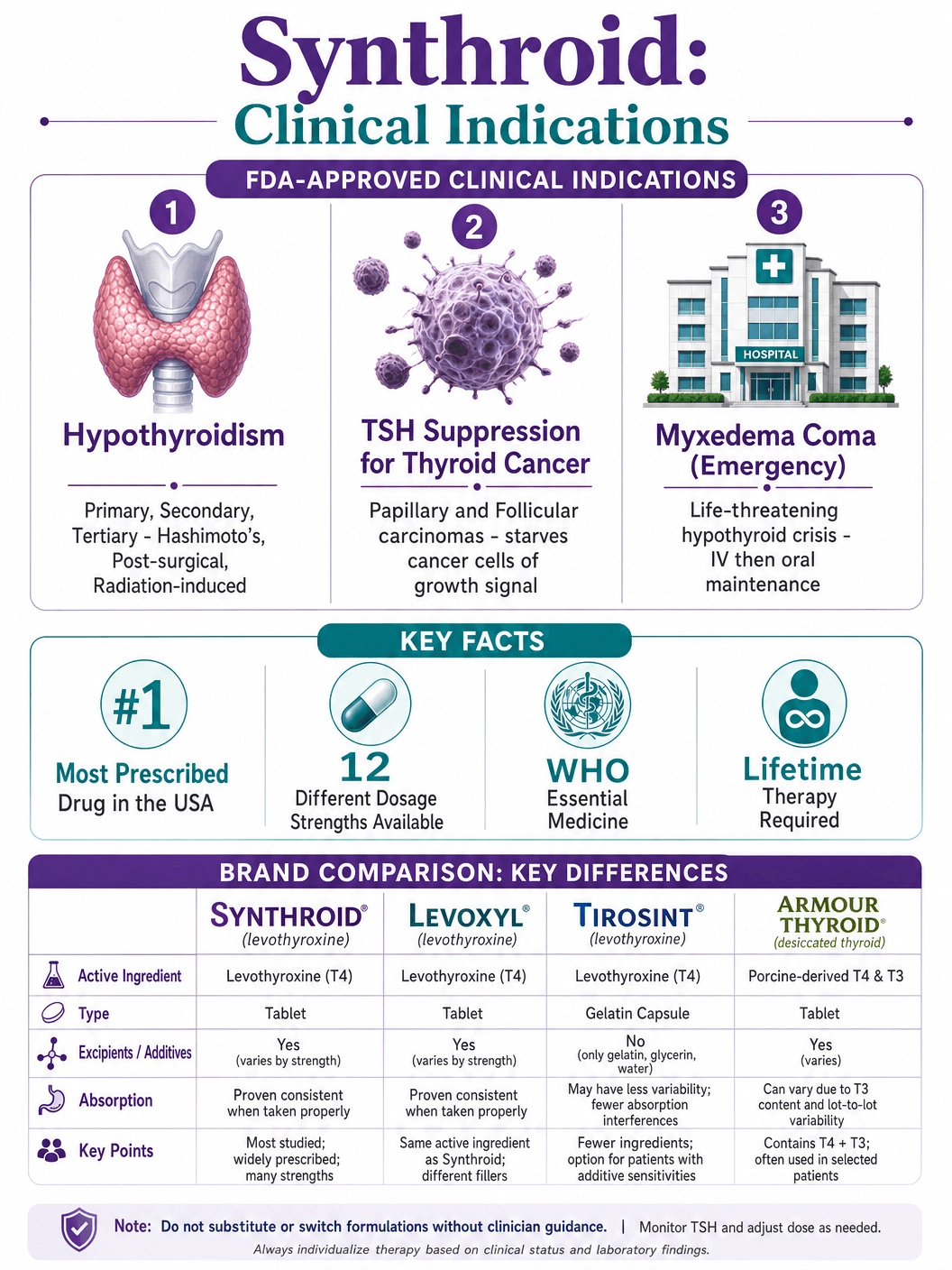
Synthroid is FDA-approved for three primary clinical indications, all related to the replacement or suppression of thyroid hormones.
Hypothyroidism: This is the most common indication. Synthroid is used as replacement therapy in primary (thyroidal), secondary (pituitary), and tertiary (hypothalamic) congenital or acquired hypothyroidism. It is the standard of care for treating Hashimoto's thyroiditis, post-surgical hypothyroidism (after thyroidectomy), and radiation-induced hypothyroidism.
Pituitary TSH Suppression: Synthroid is used in the management of well-differentiated thyroid cancer (papillary and follicular carcinomas). Because TSH stimulates the growth of thyroid tissue (including cancerous thyroid cells), high doses of Synthroid are given to artificially suppress TSH levels to near zero, thereby starving any remaining cancer cells of the growth signal they need to proliferate.
Myxedema Coma: This is a rare, life-threatening complication of severe, untreated hypothyroidism characterized by profound hypothermia, bradycardia, and altered mental status. While intravenous (IV) levothyroxine is typically used in the acute emergency setting, oral Synthroid is used for long-term maintenance once the patient is stabilized.
The Critical Importance of Proper Administration
Levothyroxine is notoriously difficult for the body to absorb. Its absorption occurs primarily in the jejunum and upper ileum of the small intestine and is highly dependent on an acidic stomach environment. Because of this, the rules for taking Synthroid are strict and must be followed meticulously to ensure consistent blood levels.
The Empty Stomach Rule: Synthroid must be taken on an empty stomach, ideally 30 to 60 minutes before breakfast, with a full glass of water. Food, particularly high-fiber foods, significantly impairs the absorption of the drug. If a patient eats immediately after taking the pill, a large percentage of the dose will pass through the digestive tract unabsorbed.
The Nighttime Alternative: For patients who struggle with the morning routine, recent studies have shown that taking Synthroid at bedtime can be equally, if not more, effective. However, the patient must have an empty stomach, meaning they cannot have eaten anything for at least 3 to 4 hours prior to taking the dose.
Consistency is Key: Whether taken in the morning or at night, the most important factor is consistency. The medication must be taken at the same time, in the same way, every single day. Even minor variations in absorption can lead to significant fluctuations in TSH levels and a return of hypothyroid symptoms.
Drug and Food Interactions: What to Avoid
Because levothyroxine absorption is so fragile, it interacts with a vast array of foods, supplements, and other medications. Patients must be vigilant about spacing out their medications.
Calcium and Iron Supplements: Calcium carbonate (found in antacids like Tums and many calcium supplements) and ferrous sulfate (iron supplements) physically bind to levothyroxine in the digestive tract, forming an insoluble complex that the body cannot absorb. These supplements must be taken at least 4 hours apart from Synthroid.
Proton Pump Inhibitors (PPIs) and Antacids: Medications that reduce stomach acid, such as omeprazole (Prilosec), esomeprazole (Nexium), and aluminum/magnesium-based antacids (Maalox, Mylanta), alter the pH of the stomach, significantly reducing the dissolution and absorption of levothyroxine.
Dietary Interferences: Certain foods are known to severely inhibit absorption. These include:
- Soy products (soy milk, tofu, edamame)
- Walnuts
- Cottonseed meal
- High-fiber diets
- Grapefruit juice (may delay absorption)
Estrogen and Birth Control: Oral contraceptives and hormone replacement therapy containing estrogen increase the levels of thyroxine-binding globulin (TBG) in the blood. TBG binds to T4, making it inactive. Therefore, women starting or stopping estrogen therapy often require an adjustment in their Synthroid dose.
Understanding the Side Effect Profile
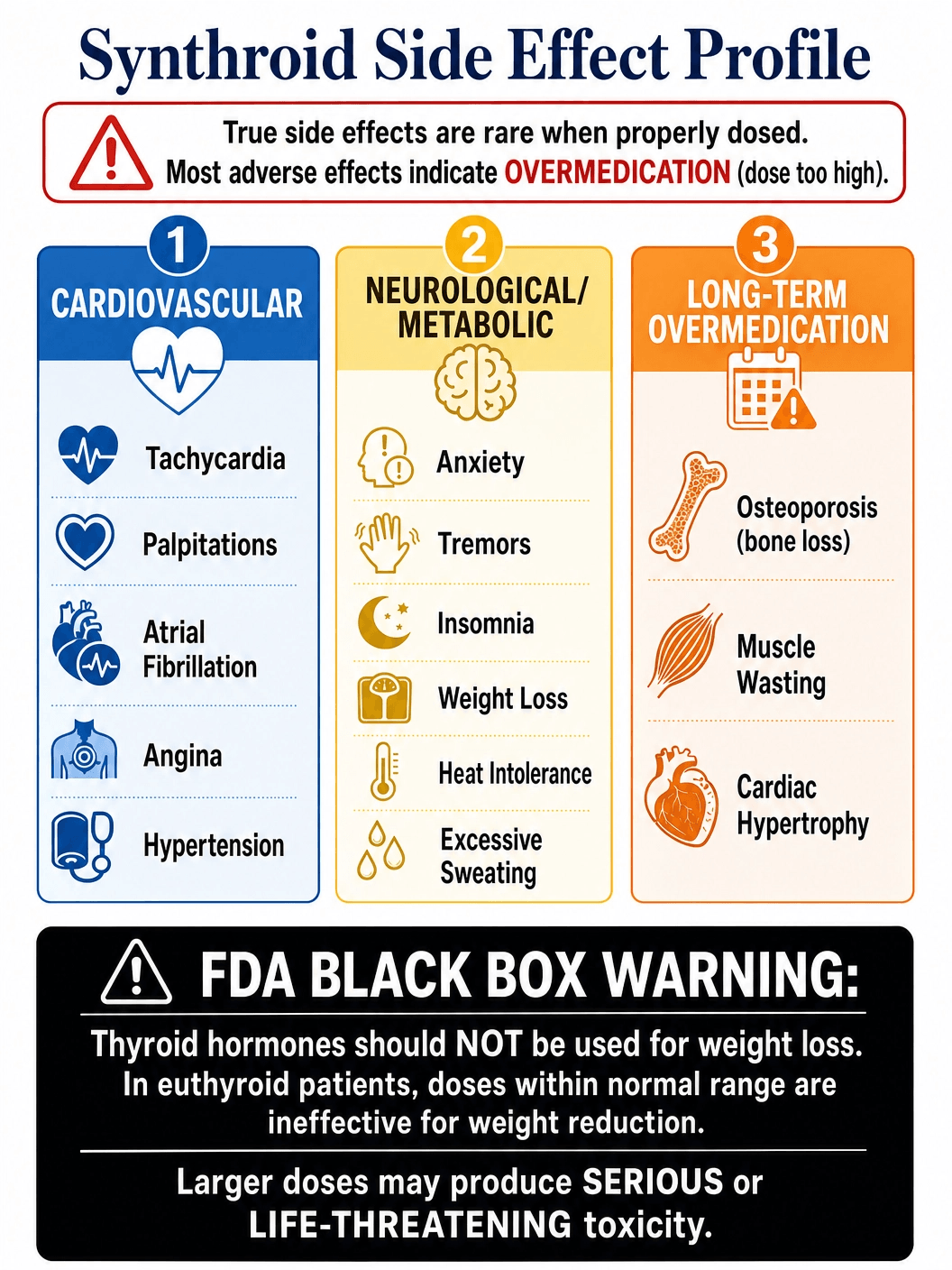
When dosed correctly, Synthroid simply replaces a hormone the body is missing, and therefore, true "side effects" are rare. Almost all adverse reactions associated with Synthroid are actually symptoms of iatrogenic (medically induced) hyperthyroidism—meaning the dose is too high.
Symptoms of Overmedication (Hyperthyroidism): If the dose of Synthroid is too high, the patient's metabolism shifts into overdrive. Symptoms include:
- Cardiovascular: Rapid heart rate (tachycardia), palpitations, arrhythmias (such as atrial fibrillation), increased blood pressure, and chest pain (angina).
- Neurological: Anxiety, nervousness, irritability, tremors (especially in the hands), and severe insomnia.
- Metabolic: Unintentional weight loss despite an increased appetite, heat intolerance, excessive sweating, and muscle weakness.
- Gastrointestinal: Diarrhea or increased frequency of bowel movements.
- Bone Health: Long-term overmedication, particularly in postmenopausal women, accelerates bone turnover, leading to decreased bone mineral density and an increased risk of osteoporosis and fractures.
The Black Box Warning: The FDA has issued a strict Black Box Warning for all levothyroxine products: Synthroid should never be used for the treatment of obesity or for weight loss. In patients with normal thyroid function, standard doses will not cause weight loss, and large doses can cause life-threatening toxicity, particularly when combined with sympathomimetic diet pills.
Available Dosages and Titration
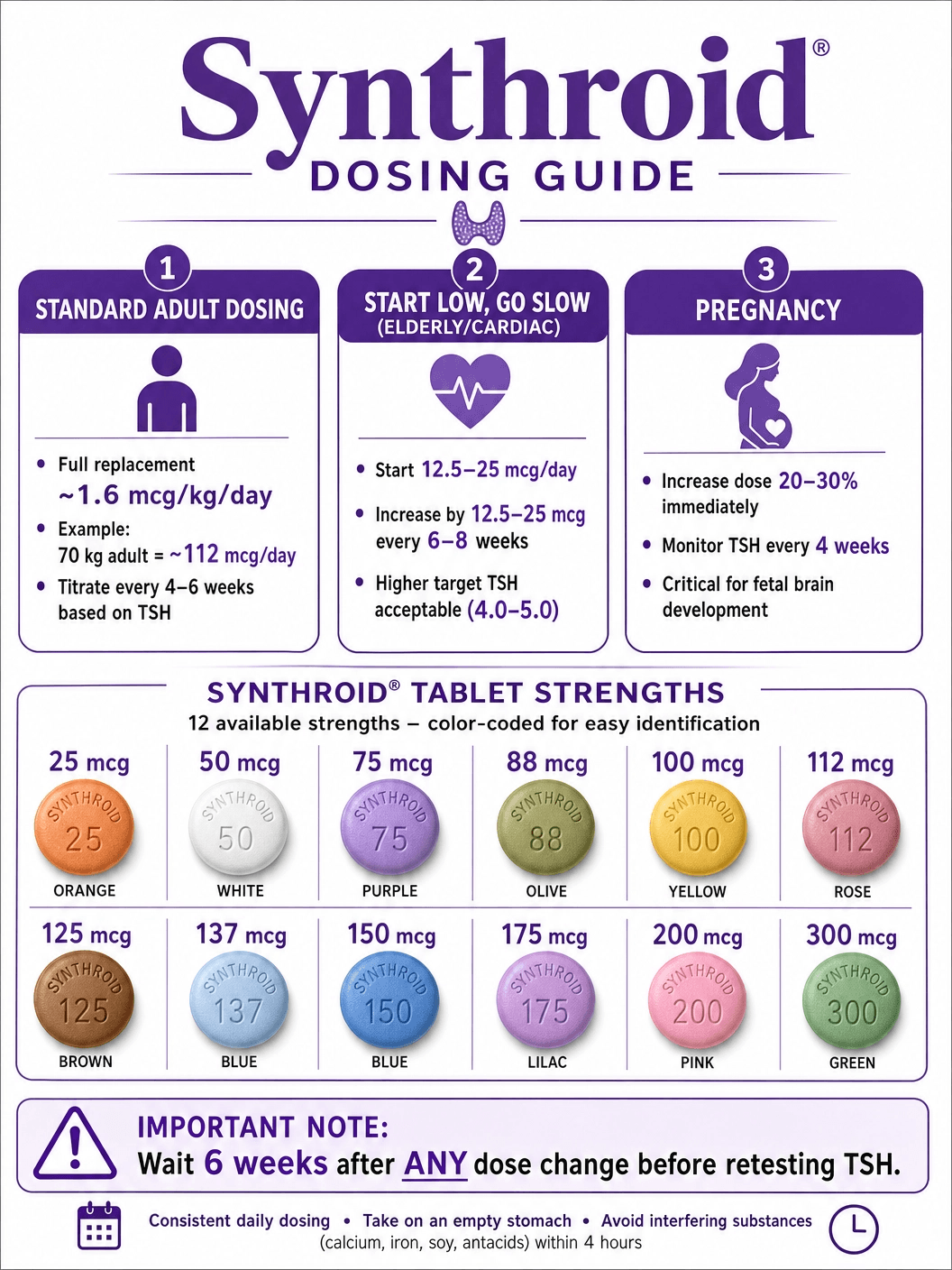
Synthroid is unique in the pharmaceutical world because it is manufactured in 12 different, highly specific dosage strengths, ranging from 25 micrograms (mcg) to 300 mcg. This wide array of options is necessary because the therapeutic window for levothyroxine is incredibly narrow; a change of just 12.5 mcg can mean the difference between feeling exhausted and feeling anxious.
Standard Adult Dosing
For a healthy adult with full hypothyroidism, the full replacement dose is typically calculated based on body weight, approximately 1.6 mcg per kilogram per day. For a 70 kg (154 lb) adult, this equates to roughly 112 mcg per day. However, physicians rarely start at the full replacement dose.
The "Start Low, Go Slow" Approach
In older adults (over 50 years of age) or patients with underlying cardiovascular disease, starting at a full replacement dose can shock the heart, potentially triggering angina or a heart attack. In these populations, the starting dose is usually very low (12.5 to 25 mcg per day). The dose is then gradually increased (titrated) every 4 to 6 weeks based on clinical symptoms and follow-up TSH blood tests.
Pregnancy Adjustments
During pregnancy, the maternal thyroid must produce enough hormone for both the mother and the developing fetus, particularly in the first trimester before the fetal thyroid is fully functional. Women taking Synthroid who become pregnant typically require a 20% to 30% increase in their dose almost immediately. Frequent TSH monitoring (every 4 weeks) is critical during pregnancy to prevent neurodevelopmental delays in the child and complications like preeclampsia or miscarriage.
Generic vs. Brand Name Synthroid: The Narrow Therapeutic Index Debate
The debate between brand-name Synthroid (manufactured by AbbVie) and generic levothyroxine is one of the most contentious issues in endocrinology. Levothyroxine is classified as a Narrow Therapeutic Index (NTI) drug, meaning small differences in dose or blood concentration can lead to serious therapeutic failures or adverse drug reactions.
The FDA Standard: The FDA requires generic drugs to demonstrate bioequivalence to the brand name, meaning the active ingredient must be absorbed at the same rate and to the same extent. For most drugs, a variance of 80% to 125% is acceptable. For NTI drugs like levothyroxine, the FDA tightened the standard to 90% to 111%.
The Clinical Reality: Despite these tightened standards, many endocrinologists and professional organizations (like the American Thyroid Association) strongly advise against switching between different manufacturers of levothyroxine. A patient stabilized on brand-name Synthroid who is switched to a generic (or switched from one generic manufacturer to another by their pharmacy) may experience a slight shift in absorption. Because the therapeutic window is so narrow, this slight shift can cause their TSH to swing out of the normal range, bringing back symptoms of hypothyroidism or causing hyperthyroidism.
The Recommendation: If a patient starts on brand-name Synthroid, they should ideally stay on brand-name Synthroid. If they start on a generic, they should try to ensure their pharmacy consistently fills the prescription with a generic from the exact same manufacturer every month. If a switch is unavoidable, the patient must have their TSH retested 6 weeks after the change to ensure the new formulation is providing the correct amount of hormone.
Purchasing Synthroid: Cost, Insurance, and Legal Acquisition
Synthroid is a prescription-only medication. It is not a controlled substance, but it requires a valid prescription from a licensed healthcare provider.
Cost and Insurance: Generic levothyroxine is extremely inexpensive, often costing less than $10 for a month's supply, and is covered as a Tier 1 generic by virtually all insurance plans. Brand-name Synthroid is significantly more expensive, often costing $40 to $60 per month out-of-pocket. Many insurance companies require a "Dispense as Written" (DAW) code from the physician and may still charge a higher copay or require prior authorization to cover the brand name over the generic.
Counterfeit Prevention: Because it is a daily maintenance medication, patients sometimes seek cheaper alternatives online. It is critical to purchase Synthroid only from reputable, licensed pharmacies. Counterfeit thyroid medication can be incredibly dangerous, as incorrect dosing can lead to severe cardiac complications or myxedema coma.
The T4 vs. T3 Debate: Desiccated Thyroid Extract
While Synthroid (T4 only) is the gold standard for hypothyroidism treatment, a subset of patients continue to experience symptoms (like fatigue, brain fog, and weight gain) despite having normal TSH levels on Synthroid. This has fueled an ongoing debate about the necessity of T3 supplementation.
The Conversion Issue: The premise of Synthroid therapy relies on the body's ability to efficiently convert the synthetic T4 into the active T3 hormone. Some researchers and patients argue that certain individuals have genetic variations (polymorphisms in the deiodinase enzymes) that make them poor converters. For these patients, T4 alone may not be sufficient.
Desiccated Thyroid Extract (DTE): Medications like Armour Thyroid or NP Thyroid are derived from the dried thyroid glands of pigs. Unlike Synthroid, DTE contains both T4 and T3 (as well as T2, T1, and calcitonin). While some patients report feeling significantly better on DTE, major endocrinology societies generally advise against its use as a first-line treatment. The ratio of T4 to T3 in pigs (4:1) is much higher than in humans (14:1), which can lead to supraphysiologic spikes in T3 levels, causing palpitations and anxiety. Furthermore, the hormone content in DTE can vary slightly from batch to batch, making it harder to maintain stable TSH levels compared to the precise, synthetic dosing of Synthroid.
Combination Therapy: For patients who fail to thrive on Synthroid alone, some endocrinologists will prescribe a combination of Synthroid (T4) and Cytomel (synthetic T3, liothyronine). This allows for precise, individualized dosing of both hormones without the variability of animal-derived extracts.
Government and Regulatory Resources
For the most accurate, up-to-date, and comprehensive information regarding Synthroid and levothyroxine, patients and healthcare professionals should consult official government and regulatory resources:
- U.S. Food and Drug Administration (FDA): The FDA provides access to the official prescribing information, safety alerts, and the Black Box Warning regarding the misuse of levothyroxine for weight loss. (fda.gov)
- National Institutes of Health (NIH) / DailyMed: DailyMed, provided by the National Library of Medicine, offers the most recent, comprehensive package inserts and labeling information submitted to the FDA. (dailymed.nlm.nih.gov)
- American Thyroid Association (ATA): While not a government body, the ATA provides the definitive clinical practice guidelines for the treatment of hypothyroidism and the use of levothyroxine. (thyroid.org)
Synthroid and the Aging Population
The management of hypothyroidism in the elderly presents unique challenges that require careful consideration and specialized dosing strategies. As the human body ages, the natural production of thyroid hormones gradually declines, and the clearance rate of these hormones from the bloodstream also slows down. Consequently, the daily requirement for levothyroxine replacement is generally lower in older adults compared to younger patients.
The Risk of Overtreatment: The most significant danger when prescribing Synthroid to elderly patients is overtreatment, leading to subclinical or overt hyperthyroidism. The aging heart is particularly sensitive to excess thyroid hormone. Even mildly elevated levels of T4 can trigger atrial fibrillation, a dangerous irregular heartbeat that significantly increases the risk of stroke. Furthermore, excess thyroid hormone accelerates bone resorption. In postmenopausal women and elderly men who are already at risk for osteoporosis, overmedication with Synthroid can lead to a rapid loss of bone mineral density and a devastating increase in the risk of hip and spinal fractures.
Conservative Dosing Protocols: Due to these risks, endocrinologists employ a highly conservative approach when initiating Synthroid in patients over the age of 65, and particularly those over 75 or with known coronary artery disease. The starting dose is often as low as 12.5 to 25 mcg per day. The dose is then titrated upward very slowly, often waiting 6 to 8 weeks between adjustments, until the TSH level normalizes. The target TSH range for elderly patients is also often adjusted upward; while a TSH of 1.5 mIU/L might be ideal for a 30-year-old, a TSH of 4.0 or even 5.0 mIU/L may be considered perfectly acceptable and safer for an 80-year-old.
The Impact of Synthroid on Mental Health and Cognition
The brain is exquisitely sensitive to thyroid hormone levels. Thyroid receptors are densely concentrated in areas of the brain responsible for mood regulation, memory, and cognitive processing, such as the hippocampus and the amygdala. Therefore, untreated hypothyroidism frequently presents with profound psychiatric and cognitive symptoms, which Synthroid is designed to reverse.
Depression and Anxiety: Hypothyroidism is a well-documented cause of secondary depression. Patients often experience profound apathy, anhedonia (loss of interest in previously enjoyed activities), and emotional flattening. Conversely, if a patient is overmedicated with Synthroid, they may experience severe anxiety, panic attacks, and emotional lability. Restoring the delicate balance of T4 and T3 with proper Synthroid dosing is often sufficient to resolve these mood disorders without the need for traditional psychiatric medications.
"Brain Fog" and Cognitive Impairment: One of the most common and frustrating complaints of hypothyroid patients is "brain fog"—a constellation of symptoms including poor concentration, short-term memory deficits, word-finding difficulties, and slowed mental processing. In severe cases, particularly in the elderly, hypothyroidism can mimic the symptoms of dementia (often referred to as "pseudodementia"). Once Synthroid therapy is initiated and TSH levels are normalized, these cognitive deficits typically reverse, though it may take several months of stable therapy for the "brain fog" to completely lift.
Synthroid in Pediatric Patients: Growth and Development
Thyroid hormone is absolutely critical for normal physical growth and neurological development in infants and children. The use of Synthroid in pediatric populations requires aggressive monitoring and frequent dose adjustments to keep pace with the child's rapid growth.
Congenital Hypothyroidism: Approximately 1 in 2,000 to 4,000 babies is born with congenital hypothyroidism, meaning they are born without a functioning thyroid gland. If left untreated, this condition leads to severe, irreversible intellectual disability (formerly known as cretinism) and stunted physical growth. Newborn screening programs test for this condition immediately after birth. If detected, Synthroid therapy must be initiated within the first two weeks of life. The starting dose for infants is relatively massive compared to adults (10 to 15 mcg/kg/day) to rapidly normalize T4 levels and protect the developing brain.
Acquired Hypothyroidism in Childhood: Children can also develop Hashimoto's thyroiditis or other forms of acquired hypothyroidism. Symptoms in children often differ from adults; rather than fatigue and weight gain, the primary signs are often a sudden cessation of linear growth (falling off the growth chart), delayed puberty, and declining academic performance. Synthroid therapy restores normal growth velocity and allows for normal pubertal development. Because children metabolize levothyroxine faster than adults, their weight-based dose requirements are higher and must be recalculated frequently as they grow.
The Pharmacokinetics of Levothyroxine
Understanding how the body processes Synthroid (its pharmacokinetics) is essential for explaining why the medication must be taken so precisely and why it takes so long to see clinical results.
Absorption: As previously noted, levothyroxine absorption is highly variable, ranging from 40% to 80% of the administered dose. It occurs primarily in the small intestine and is heavily dependent on an acidic fasting state. Peak blood concentrations are typically reached 2 to 4 hours after oral ingestion.
Distribution and Protein Binding: Once in the bloodstream, over 99% of levothyroxine is immediately bound to plasma proteins, primarily thyroxine-binding globulin (TBG), transthyretin, and albumin. Only the tiny fraction of "free" or unbound hormone (less than 0.1%) is metabolically active and available to enter cells. This high degree of protein binding acts as a massive reservoir, buffering the body against sudden changes in hormone levels.
Metabolism and Half-Life: The primary pathway for levothyroxine metabolism is sequential deiodination. Enzymes in the liver and kidneys remove iodine atoms from the T4 molecule, converting it either into the active T3 hormone or into inactive reverse T3 (rT3). The most remarkable pharmacokinetic feature of levothyroxine is its exceptionally long half-life of 6 to 7 days in a normal individual (and up to 9 to 10 days in a hypothyroid patient). Because of this long half-life, it takes approximately 4 to 6 weeks of daily dosing for the drug to reach a "steady state" in the bloodstream. This is why physicians must wait at least 6 weeks after changing a Synthroid dose before retesting the TSH level; testing any sooner will not accurately reflect the full effect of the new dose.
Managing Hypothyroidism During Surgery and Illness
Acute illness, trauma, and surgical procedures place significant stress on the body and can alter thyroid hormone dynamics, requiring careful management of Synthroid therapy.
Euthyroid Sick Syndrome: During severe acute illness (such as sepsis, major trauma, or admission to the ICU), the body intentionally downregulates its metabolism to conserve energy. It does this by decreasing the conversion of T4 to active T3, and increasing the conversion of T4 to inactive reverse T3. This results in low T3 levels, normal or low T4 levels, and normal or low TSH levels—a condition known as Euthyroid Sick Syndrome or Non-Thyroidal Illness Syndrome. In these cases, the thyroid gland itself is fine, and administering extra Synthroid is generally not recommended and can actually be harmful. The hormone levels will normalize once the underlying illness resolves.
Perioperative Management: For patients with established hypothyroidism who are scheduled for elective surgery, it is crucial that they are clinically euthyroid (normal TSH) prior to the procedure. Untreated hypothyroidism increases the risk of intraoperative complications, including hypotension, heart failure, delayed recovery from anesthesia, and postoperative ileus (paralysis of the bowel). Because Synthroid has a 7-day half-life, missing a single dose on the morning of surgery (due to NPO/fasting status) is clinically insignificant. However, if a patient is unable to take oral medications for several days post-surgery, intravenous (IV) levothyroxine may be administered, typically at 50% of the patient's usual oral dose, as IV administration bypasses the digestive tract and is 100% absorbed.
The Future of Thyroid Replacement Therapy
While Synthroid has been the standard of care for decades, ongoing research is exploring new avenues for thyroid hormone replacement, particularly for the subset of patients who remain symptomatic on T4 monotherapy.
Liquid and Gel Cap Formulations: To combat the severe absorption issues associated with traditional levothyroxine tablets, pharmaceutical companies have developed liquid solutions (e.g., Tirosint-SOL) and soft gel capsules (e.g., Tirosint). These formulations do not require stomach acid for dissolution and are significantly less affected by food, coffee, or interacting medications like PPIs. They offer a more stable and predictable absorption profile, though they are currently much more expensive than standard tablets.
Sustained-Release T3: The main problem with combining Synthroid (T4) with Cytomel (T3) is that T3 has a very short half-life (about 1 day) and is rapidly absorbed, causing a sudden spike in blood levels that can cause palpitations, followed by a rapid drop. Researchers are currently developing sustained-release formulations of T3 that would mimic the thyroid gland's slow, continuous release of the active hormone, potentially offering a safer and more effective combination therapy for patients with genetic conversion defects.
Regenerative Medicine: In the distant future, the ultimate treatment for hypothyroidism may not be a daily pill at all. Scientists are exploring the use of stem cells to grow functional thyroid tissue in the lab, which could theoretically be implanted into a patient to restore natural, autoregulated hormone production, effectively curing the disease.
Synthroid and Weight Management: Dispelling the Myths
One of the most pervasive and dangerous myths surrounding Synthroid is its association with weight loss. Because hypothyroidism is famously associated with a slowed metabolism and weight gain, many patients mistakenly believe that taking Synthroid will act as a magic bullet for shedding excess pounds. This misconception requires careful clinical clarification.
The Reality of Hypothyroid Weight Gain: When the thyroid gland fails, the basal metabolic rate (BMR) drops. However, the weight gain directly attributable to hypothyroidism is usually modest—typically only 5 to 10 pounds. Furthermore, this weight is rarely pure adipose tissue (fat). Instead, the lack of thyroid hormone causes an accumulation of mucopolysaccharides in the tissues, which trap water. Therefore, the majority of the weight gained in severe hypothyroidism is actually myxedema (a specific type of water retention) rather than fat.
What Happens When Synthroid is Started: When a hypothyroid patient begins Synthroid therapy, the medication restores the basal metabolic rate to normal and promotes the excretion of the trapped water. Consequently, patients often experience a rapid initial weight loss of a few pounds as the myxedema resolves. However, once the TSH level is normalized and the patient is euthyroid, Synthroid will not cause further weight loss. It simply levels the playing field, allowing the patient to lose weight through diet and exercise at the same rate as someone with a naturally functioning thyroid.
The Danger of Intentional Overmedication: Driven by the desire for weight loss, some patients may intentionally take more Synthroid than prescribed, or individuals with normal thyroid function may illegally acquire the drug to use as a diet pill. This is incredibly dangerous. As highlighted by the FDA's Black Box Warning, using levothyroxine for weight loss in euthyroid individuals is ineffective at standard doses. To achieve weight loss, massive, toxic doses are required. This induces a state of thyrotoxicosis, which forces the body to burn muscle mass (catabolism) rather than just fat, and places immense, potentially fatal stress on the cardiovascular system, leading to arrhythmias, cardiac hypertrophy, and sudden cardiac death.
The Impact of Environmental Disruptors on Thyroid Function
In the modern world, the thyroid gland is increasingly under assault from environmental chemicals known as endocrine-disrupting chemicals (EDCs). For patients relying on Synthroid, understanding these disruptors is crucial, as they can interfere with the medication's efficacy and the body's overall hormonal balance.
Halogens: Fluoride, Chlorine, and Bromine: The thyroid gland requires iodine to synthesize natural T4 and T3. However, iodine belongs to a family of elements called halogens, which also includes fluorine, chlorine, and bromine. Because these elements are chemically similar, they can compete with iodine for uptake into the thyroid gland. High exposure to fluoridated water, chlorinated pools, or brominated flame retardants (found in furniture and electronics) can displace iodine, exacerbating hypothyroid symptoms and potentially increasing the required dose of Synthroid.
Perchlorate: Perchlorate is a chemical used in rocket fuel, fireworks, and explosives, and it has heavily contaminated the groundwater and food supply in certain regions. Perchlorate is a potent competitive inhibitor of the sodium-iodide symporter (NIS), the mechanism the thyroid uses to pull iodine from the blood. By blocking iodine uptake, perchlorate directly suppresses thyroid function.
Bisphenol A (BPA) and Phthalates: Found in hard plastics, water bottles, and the lining of canned foods, BPA and phthalates are notorious endocrine disruptors. Studies suggest that these chemicals can bind to thyroid hormone receptors in the body's cells, acting as antagonists. This means they block the receptor, preventing the active T3 hormone (converted from Synthroid) from entering the cell and doing its job, leading to cellular hypothyroidism even if blood tests show normal hormone levels.
Synthroid and the Gastrointestinal Microbiome
Emerging research is uncovering a profound connection between the gut microbiome and thyroid health, a relationship that significantly impacts patients taking Synthroid.
The Gut-Thyroid Axis: The gastrointestinal tract is not just a digestive organ; it is a massive endocrine and immune organ. In patients with Hashimoto's thyroiditis (the leading cause of hypothyroidism), there is a high prevalence of gut dysbiosis—an imbalance of good and bad bacteria. This dysbiosis contributes to "leaky gut" (intestinal permeability), allowing undigested proteins and bacterial endotoxins to enter the bloodstream, triggering systemic inflammation and exacerbating the autoimmune attack on the thyroid gland.
Microbial Deiodination: The conversion of Synthroid (T4) to the active T3 hormone occurs primarily in the liver and kidneys, but approximately 20% of this conversion happens in the gastrointestinal tract, facilitated by an enzyme called intestinal sulfatase, which is produced by healthy gut bacteria. If a patient has a severely compromised microbiome (due to poor diet, chronic stress, or frequent antibiotic use), this intestinal conversion is impaired. Consequently, the patient may struggle to achieve optimal T3 levels despite taking an adequate dose of Synthroid.
Absorption Issues and Celiac Disease: There is a well-documented genetic link between autoimmune thyroid disease and Celiac disease (an autoimmune reaction to gluten). In patients with undiagnosed Celiac disease, the villi of the small intestine are flattened and destroyed, drastically reducing the surface area available for drug absorption. These patients often require massive, unusually high doses of Synthroid just to maintain normal TSH levels. Once a strict gluten-free diet is adopted and the intestinal lining heals, their Synthroid requirement typically drops significantly, requiring careful monitoring to prevent sudden hyperthyroidism.
Navigating the Challenges of Thyroid Testing
The management of Synthroid therapy relies entirely on accurate blood testing. However, interpreting these tests is not always straightforward, and patients must understand the nuances of thyroid panels.
The TSH Controversy: The Thyroid-Stimulating Hormone (TSH) test is the gold standard for monitoring Synthroid therapy. However, the "normal" reference range for TSH is a subject of intense debate. Most laboratories define normal as approximately 0.4 to 4.5 mIU/L. However, many functional medicine practitioners and progressive endocrinologists argue that this range is too broad, noting that healthy individuals without thyroid disease typically have a TSH between 1.0 and 2.0 mIU/L. Consequently, a patient with a TSH of 4.0 may be told their labs are "normal," even though they are still experiencing severe hypothyroid symptoms. Optimizing Synthroid therapy often requires treating the patient's symptoms, not just the lab numbers, aiming for a narrower, optimal TSH target.
Free T4 and Free T3: While TSH measures the pituitary's signal, Free T4 and Free T3 tests measure the actual amount of unbound, active hormone available in the blood. Measuring "Total" T4 or T3 is generally useless, as it includes the 99% of hormone that is bound to proteins and unavailable to cells. For patients who remain symptomatic on Synthroid despite a normal TSH, testing Free T3 is crucial to determine if the body is successfully converting the synthetic T4 into the active hormone.
Biotin Interference: A critical, often overlooked issue in thyroid testing is the interference of Biotin (Vitamin B7). Biotin is a highly popular supplement taken for hair, skin, and nail growth. However, the chemical assays used by most laboratories to measure TSH, Free T4, and Free T3 rely on a biotin-streptavidin binding mechanism. High levels of biotin in the patient's blood will physically interfere with the assay, causing falsely low TSH readings and falsely high Free T4/T3 readings. This can lead a physician to mistakenly conclude that a patient is overmedicated and incorrectly lower their Synthroid dose. Patients must stop taking all biotin supplements at least 3 to 5 days before any thyroid blood test.
Synthroid Quick View
| Manufacturer | AbbVie |
|---|---|
| Type | Synthetic Thyroid Hormone (T4) |
| Prescription | Required |
| Pregnancy Category | Category A (Safe and necessary during pregnancy) |
| Alcohol Interaction | No direct interaction, but may affect absorption if taken together |
Synthroid Side Effects
Common Side Effects
- Weight loss
- Increased appetite
- Heat intolerance
- Excessive sweating
- Headache
Uncommon Side Effects
- Tremors
- Nervousness or anxiety
- Insomnia
- Diarrhea
- Menstrual irregularities
Rare Side Effects
- Chest pain (angina)
- Rapid or irregular heartbeat (arrhythmia)
- Shortness of breath
- Seizures
Important Warning: BLACK BOX WARNING: Not for treatment of obesity or for weight loss. In euthyroid patients, doses within the range of daily hormonal requirements are ineffective for weight reduction. Larger doses may produce serious or even life-threatening manifestations of toxicity.
More Information About Synthroid
Storage
Store at room temperature away from moisture and heat. Protect from light.
Contraindications
Drug Interactions
Synthroid FAQs
Written and Reviewed by Our Qualified Team

Find out more about our medical content authors and how we ensure the accuracy of our content.
Content last updated: 23 May 2024
Synthroid Reviews
Based on 35 reviews
Synthroid has been a reliable part of my daily routine. It helps me manage my thyroid issues effectively.
I\'ve experienced helpful results with Synthroid. It has helped to restore my weight.
This medication is positive impact. I feel so much better since starting it. My energy levels are back to normal..
After trying a few different options, Synthroid is the one that truly made a difference for me. My thyroid levels are finally in a healthy range.. However, I\'m still struggling with thyroid levels.
Synthroid has been a easy to take part of my daily routine. It helps me manage my hypothyroidism effectively.
This medication is okay. I feel so much a bit better since starting it. I no longer feel constantly tired.. However, I\'m still struggling with thyroid levels.
I\'ve experienced no side effects results with Synthroid. It has helped to regulate my thyroid levels.
Synthroid has really made a difference my life. I used to feel sluggish, but now I feel optimistic.
Synthroid has been a energizing part of my daily routine. It helps me manage my thyroid issues effectively.
I was skeptical at first, but Synthroid has proven to be average. My mood is much better.
Synthroid has been a life-changing part of my daily routine. It helps me manage my low thyroid effectively.
This medication is average. I feel so much better since starting it. I still have some dry skin issues..
For anyone dealing with thyroid issues, Synthroid is definitely worth considering. It has been helpful for me.
For anyone dealing with underactive thyroid, Synthroid is definitely worth considering. It has been no side effects for me.
Synthroid has really changed my life. I used to feel unwell, but now I feel energized.
This medication is positive impact. I feel so much better since starting it. I feel like myself again..
For anyone dealing with low thyroid, Synthroid is definitely worth considering. It has been reliable for me.
After trying a few different options, Synthroid is the one that truly improved for me. I still have some dry skin issues..
I\'ve experienced helpful results with Synthroid. It has helped to restore my hair loss.
Synthroid has really helped my life. I used to feel unwell, but now I feel more stable.
I\'ve experienced average results with Synthroid. It has helped to balance my skin dryness.
This medication is consistent. I feel so much better since starting it. My concentration has improved dramatically..
Synthroid has really made a difference my life. I used to feel anxious, but now I feel energized.
For anyone dealing with low thyroid, Synthroid is definitely worth considering. It has been positive impact for me.
Synthroid has really improved my life. I used to feel a bit off, but now I feel optimistic.
I\'ve experienced positive impact results with Synthroid. It has helped to regulate my energy levels.
Synthroid has been a improved part of my daily routine. It helps me manage my underactive thyroid effectively.
Synthroid has really transformed my life. I used to feel a bit off, but now I feel balanced. However, I\'ve noticed some headaches.
Synthroid has really improved my life. I used to feel sluggish, but now I feel balanced.
Synthroid has been a life-changing part of my daily routine. It helps me manage my low thyroid effectively.
I was skeptical at first, but Synthroid has proven to be effective. My thyroid levels is much better.
Initially, I was hopeless, but after some time on Synthroid, I\'m feeling healthier.
I\'ve been taking Synthroid for a while now and it has been reliable. My concentration has almost gone.
I\'ve been taking Synthroid for a while now and it has been effective. My overall well-being has significantly improved.
For anyone dealing with thyroid issues, Synthroid is definitely worth considering. It has been manageable for me. However, I\'ve noticed some digestive issues.
Leave a Review
How Does It Work?
Research
Read our comprehensive review to understand the medication
Consult Your Doctor
Discuss the medication with your healthcare provider
Get Your Prescription
Obtain a valid prescription from your doctor